1.Introduction
Healthcare disparities continue to be a significant challenge in modern healthcare systems, leading to inequities in access, quality of care, and health outcomes across different populations. These inequities disproportionately affect marginalized groups, including individuals from lower socioeconomic backgrounds, racial and ethnic minorities, and those with limited health literacy. Addressing healthcare inequities requires a comprehensive understanding of the root causes of these disparities. As future healthcare providers, student nurses are in a critical position to influence and shape equitable healthcare. By understanding the social, economic, and systemic factors that contribute to healthcare inequities, student nurses can become advocates for change within the healthcare system.
The persistence of healthcare inequities is well-documented, with significant disparities in access to healthcare services, quality of care, and health outcomes across different socioeconomic, racial, and ethnic groups.[1] Socioeconomic status (SES) plays a pivotal role in shaping health outcomes. Individuals from lower SES backgrounds often face barriers to healthcare, including financial constraints, lack of insurance, and limited access to healthcare facilities. These barriers result in poorer health outcomes, including higher rates of chronic illness, delayed care, and lower life expectancy.[2]
Systemic racism is another key contributor to healthcare inequities. Marginalized racial and ethnic groups often experience discrimination within the healthcare system, resulting in unequal treatment, biased clinical decision-making, and disparities in care access.[3] These groups are more likely to experience poor disease management, inadequate pain control, and worse health outcomes compared to their white counterparts. Addressing racism in healthcare requires both systemic reforms and individual awareness among healthcare providers. Health literacy, the ability to understand and use health information to make informed decisions, is also a critical factor in healthcare inequities. Individuals with limited health literacy often need help navigating the complexities of the healthcare system, engaging in preventive health behaviors, and adhering to treatment plans. This lack of health literacy can lead to miscommunication between patients and providers, non-adherence to medical advice, and worse health outcomes.[4]
Given the significance of these root causes, student nurses need to develop a comprehensive understanding of healthcare inequities and the factors that perpetuate them. As future healthcare providers, student nurses will encounter diverse populations with varying needs, and their ability to recognize and address these inequities will directly impact the quality of care they provide. By exploring student nurses’ perceptions of healthcare disparities, this study sheds light on students’ awareness of these inequities during their professional formation.
Despite efforts to achieve equitable healthcare, significant disparities in access, quality, and health outcomes continue to affect marginalized populations. For future healthcare professionals, particularly student nurses, understanding the complex network of social, economic, and structural root causes of these disparities is essential to shaping more equitable healthcare practices and policies. However, more information is needed to understand how student nurses perceive the factors contributing to healthcare inequities. This study seeks to address this gap by exploring student nurses’ perceptions of the root causes of healthcare disparities. Nursing students’ perceptions are critical to informing educational strategies and promoting a healthcare workforce equipped to address disparities in clinical practice. Understanding these perceptions may lead to enhanced curricula and the development of interventions that foster more socially conscious healthcare providers committed to reducing healthcare inequities. Identifying how student nurses understand and perceive the social determinants of health (SDOH) will provide valuable insights into their preparedness to address healthcare disparities in clinical practice. The findings from this research will inform nursing education programs, equipping future nurses with the knowledge and skills needed to promote health equity in diverse populations.
2.Methods
The study was conducted at a four-year public university and surveyed its School of Nursing students. All student nurses enrolled in the nursing program were invited to participate, ensuring a broad representation of perspectives on healthcare inequities and enriching the research findings with diverse backgrounds and experiences. To note, we adhered to compliance protocols to protect all student nurses involved in the study, and the academic institution’s IRB approved the study. Quantitative survey data were analyzed using descriptive statistics (mean, standard deviation, and frequency). Responses were transcribed and analyzed qualitatively using thematic analysis to identify recurring themes and patterns.
The survey was distributed online through the nursing school’s listserv and supported by strategically placed flyers in common student areas. Faculty were informed about the study and encouraged their students to participate. Participants received a $10 gift card to complete the survey. Two faculty members, one from the Nursing department and the other from the Medical Humanities department, developed the survey questions based on key themes, including socioeconomic status, systemic racism, and health literacy. The survey questions were: What are student nurses’ perceptions regarding the underlying causes and contributors to healthcare disparities? What are student nurses’ perceptions of health care disparities regarding access to care based on socioeconomic factors? What are the attitudes and beliefs of student nurses regarding the impact of implicit bias on healthcare disparities? How do student nurses perceive healthcare disparities in terms of racial and ethnic disparities in health outcomes? Do student nurses’ perceptions of healthcare disparities evolve over the four years of their nursing education? The goal was to identify knowledge gaps and enhance educational strategies that prepare student nurses to effectively address and reduce healthcare inequities in their future practice.
Each student completed an online survey containing questions to yield qualitative and quantitative data. The survey included a section that asked participants to take the Implicit Association Test (IAT). The IAT measures implicit biases, unconscious attitudes, or associations individuals may hold. It assesses how quickly a person associates different concepts (e.g., race, gender) with positive or negative attributes.[5] Widely used in research on bias and social psychology, the IAT has both strengths and weaknesses. The test can be adapted to measure biases across domains such as race, gender, disability, age, and preferences for specific products. Its flexibility allows the researchers to explore implicit attitudes across different contexts. The IAT is a valuable tool for raising awareness of implicit biases and exploring unconscious attitudes across other areas of human behavior.[6] However, because of its weaknesses in reliability and susceptibility to external influences, the IAT was used judiciously in this study, in conjunction with other methods, to understand students’ awareness of bias in a nuanced and comprehensive manner. For this IAT, students were asked to categorize faces and positive and negative words racially. Finally, the students described their understanding, awareness, attitudes, and beliefs regarding the root causes of healthcare disparities through a combination of structured survey items and open-ended questions. In addition to quantitative measures, the survey included open-ended prompts that allowed students to describe, in their own words, their perceptions and understanding of healthcare disparities. These qualitative responses were used to capture nuance, context, and depth of understanding that may not be fully reflected in closed-ended items.
This study also used the Social Ecological Model (SEM), which highlights how individual, interpersonal, community, and societal factors shape health outcomes, emphasizing that personal behaviors and environmental conditions influence health.[7] At the individual level, student nurses’ perceptions were shaped by their knowledge and attitudes toward health disparities. Interpersonal factors such as family and peer relationships influence their behavior and understanding of SDOH. On a broader scale, community resources like healthcare access and socioeconomic opportunities play critical roles in shaping health outcomes.[8]
Societal structures, policies, and cultural norms significantly influence individuals’ and populations’ access to resources. In nursing education, the SEM is instrumental in examining how student nurses’ education and experiences shape their perspectives on SDOH. Factors such as curricula, clinical exposure, and societal norms impact their understanding of health inequities and their underlying causes.[9] This framework emphasizes the need for a comprehensive approach to addressing SDOH across various levels,[10] highlighting the complexity of tackling health disparities. By considering individual experiences, educational backgrounds, and societal contexts, we gain deeper insights into how future nurses can effectively address systemic health inequities in their professional practices.
3.Results
The findings illustrate a comprehensive awareness of the systemic issues driving healthcare disparities. The emphasis on economic challenges, educational inequalities, and geographic factors highlights students’ recognition of the complex interplay of social determinants shaping health outcomes. The study population comprised 187 School of Nursing students: 40 seniors, 35 juniors, 55 sophomores, and 57 freshmen. Most respondents (79%) were between 18 and 24 years old, aligning with the study’s demographic of undergraduate students. A smaller portion (11%) fell within the 25-34 age group, while minimal representation in other age categories (2%-4%). The gender distribution showed that 87% identified as women, 13% as men, and no other gender identities were disclosed. Regarding sexual orientation, 87% identified as heterosexual, with smaller proportions identifying as homosexual or bisexual (4% each), or questioning/prefer not to say (2% each). The survey’s ethnic breakdown indicated that 54% of respondents were White, 20% Black/African American, 13% Asian, and 7% Mixed/Biracial.
The response rate was 24%. There were 6 respondents among 57 total freshmen (11%) and 7 among 55 total sophomores (13%). There were 24 respondents out of 35 total juniors, representing the largest group (69%) and suggesting a greater likelihood of survey participation among this cohort. Seniors comprised 8 respondents of 40 total seniors (20%), including students nearing graduation. The distribution shows varied representation across all class years, with a notable concentration in the junior year, suggesting differing perspectives and experiences at each stage of the nursing program.
Based on the Centers for Disease Control’s definition of health disparities, the students were asked about their familiarity with the concept. Students’ familiarity with health disparities was assessed using researcher-developed survey questions included in the study’s survey questionnaire, designed to capture self-reported familiarity with those key concepts. Familiarity with the Concept of Health Disparities (see Figure 1): Not familiar at all: 2% (1 respondent), Slightly familiar: 2% (1 respondent), Moderately familiar: 32% (14 respondents), Very familiar: 48% (21 respondents), Extremely familiar: 16% (7 respondents). About 48% of respondents are very familiar with health disparities, and an additional 16% are extremely familiar. This indicates that the majority (64%) of participants strongly understand the topic, which suggests that most in the group have knowledge or understanding of health disparities. 32% of respondents report being moderately familiar with the concept, indicating a baseline understanding but potentially an opportunity to deepen their knowledge.
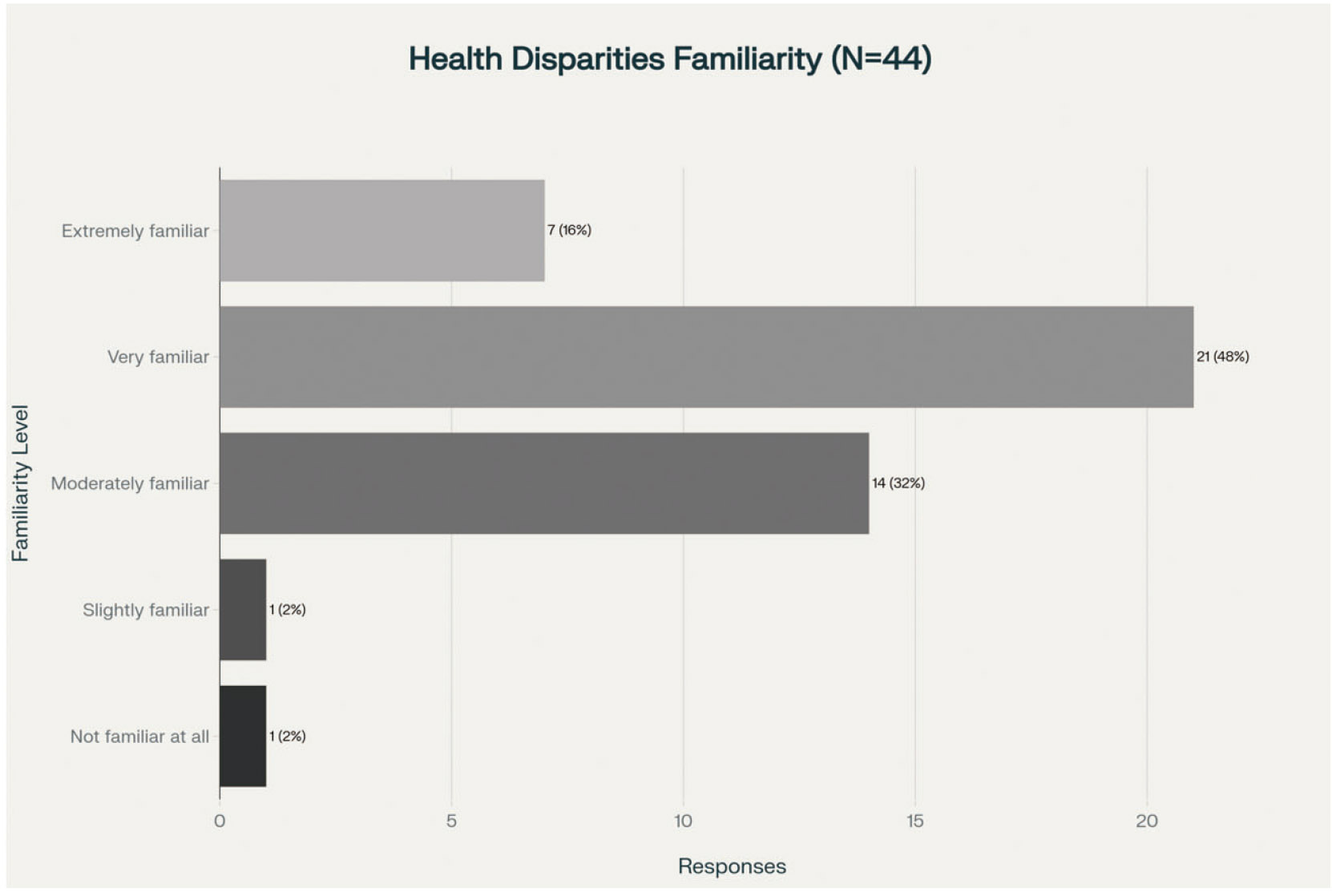
Figure 1.
Health disparities familiarity
This group may benefit from further education on how health disparities affect different populations. Only a small fraction of respondents are slightly familiar (2%) or unfamiliar (2%) with health disparities. This suggests that very few respondents are entirely unaware of this issue, reflecting a general awareness. Forty-four respondents answered this question. The overwhelming majority (98%) are at least somewhat familiar with health disparities, indicating that this topic is relevant to respondents’ knowledge base through their engagement with public health or nursing education.
3.1Instructions on healthcare disparities
Key themes emerged from qualitative open-ended questions about students’ exposure to healthcare disparities in their nursing education. Most respondents reported learning about these issues through formal coursework, including:
- Ethics and Policy Classes: These courses covered cultural competence and the impact of social determinants on health.
- Introduction to Nursing Courses: Basic concepts of healthcare disparities were introduced early, emphasizing awareness of healthcare gaps.
- Community and Public Health: Courses such as Population & Community Health, Global Health, and Community Health, often paired with clinical experiences, provided practical insights into healthcare disparities.
- Nursing Research: Students referenced research-focused courses that explored healthcare disparities, through healthcare policy and genetics research.
- Public Health Background: Respondents had prior educational experiences outside of nursing, such as degrees in public health, where they received extensive training on healthcare disparities. Students were exposed to the subject in more depth before entering their nursing program.
Cultural competency training was a prominent method for teaching about healthcare disparities, integrated into both formal coursework and certification programs. This training focused on equitable treatment and addressing biases in care. Students also gained knowledge through informal class discussions, often tied to broader topics like ethics or specific healthcare issues. They also heard from guest speakers and received real-world insights through job training.
3.2Responses to levels of exposure to SDOH training
Students’ familiarity with SDOH was assessed using researcher-developed questions administered through a Qualtrics survey designed by the research team. When asked about their exposure to training on SDOH during the nursing program, students reported varying levels of education:
- 24% of respondents highlighted extensive exposure via multiple courses, clinical experiences, research projects, and specific certification programs focused on healthcare disparities.
- Most students (67%) indicated moderate exposure to topics such as ethics and community health through class discussions, modules, or integrated topics within other courses.
- A small group (9%) reported limited to minimal exposure to healthcare disparities, often because they had only recently started the program or had yet to encounter substantial coursework.
Most nursing students reported receiving training on healthcare disparities through formal coursework, cultural competency training, and clinical experiences. The depth of training varies, with some students participating in comprehensive research and practical applications while others have encountered only brief discussions. Cultural competence and social determinants of health are integrated throughout the curriculum at different stages of the Nursing School program.
3.3Factors contributing to healthcare disparities
Participants were asked to identify the top five factors contributing to healthcare disparities, revealing several vital issues that shape health outcomes across different populations. The most frequently cited factor was low income (see Table 1), with 88% (28 respondents) identifying it as a major contributor, emphasizing the vital link between financial resources and health outcomes. Economic challenges can limit access to essential services and preventive care, underscoring the role of economic factors in healthcare disparities. 72% of respondents (23 students) highlighted access to care as a significant barrier to seeking medical services. 63% (20 respondents) noted a lack of health coverage, indicating the role of health insurance in accessing adequate medical care and reducing vulnerability to health issues.
| Poor Access to Care | 23 |
| Low Income | 28 |
| No Health Coverage | 20 |
| Poor Education | 15 |
| Zip Code (Neighborhood) | 13 |
| Bad Health Behaviors | 4 |
| Poverty | 18 |
| Inadequate Housing | 7 |
| Unemployment or Underemployment | 14 |
| Poor Access to Healthy Foods | 12 |
| Bias or Discrimination | 16 |
| Pollution | 3 |
| Other |
Poor education was another significant factor, with 47% (15 respondents) recognizing its influence. Educational disparities often affect health literacy, impacting individuals’ ability to make informed decisions about their health. 41% (13 respondents) highlighted geographic location (i.e., zip code) as a determinant of health, underscoring how living in certain areas can affect access to healthcare services, resources, and overall health outcomes. Other factors mentioned included poverty (56%), bias or discrimination (50%), unemployment or underemployment (44%), poor access to healthy foods (38%), inadequate housing (22%), destructive health behaviors (13%), and pollution (9%). These responses suggest students’ understanding of the various social determinants impacting health.
3.4Students’ responses on the impact of healthcare disparities on patient outcomes
Students identified several significant impacts in response to the question regarding how healthcare disparities affect patient outcomes and health within their local community. The results revealed a consensus on the detrimental effects of these disparities on health and well-being. The most frequently cited impact was that healthcare disparities worsen patients’ health, with 90% of respondents (28 individuals) selecting this option. This indicates a strong belief that healthcare access and quality inequalities directly contribute to poorer health outcomes for affected individuals. The responses also indicated that healthcare disparities lower quality of life, with 87% of students (27 respondents) noting this impact. Other significant responses included that healthcare disparities exacerbate illness, with 87% of students (27 respondents). This underscores the grave long-term consequences that healthcare disparities can have on individuals, potentially leading to premature deaths within marginalized populations.
Additionally, shortening life expectancy was highlighted by 74% of participants (23 respondents) and led to patients’ distrust of healthcare professionals, 74% (23 respondents). This distrust can create barriers to seeking care, further perpetuating healthcare disparities. Lastly, 48% of participants (15 respondents) reported that disparities lead to no or minimal routine visits to healthcare professionals, highlighting the cycle of neglect in preventive care among affected communities. The findings demonstrate students’ awareness of how healthcare disparities negatively affect patient outcomes and community health.
3.5Student responses on measures to reduce healthcare disparities
Students identified key strategies when asked about the most important measures to reduce healthcare disparities in their local community. The survey results strongly agreed on the need for targeted interventions to address these disparities. The most frequently selected measure was greater access to care (see Figure 2), chosen by 72% of participants (23 respondents). Another crucial measure identified by students was access to healthcare education resources, with 69% of respondents (22 individuals) emphasizing its importance. This suggests an understanding that educational initiatives can help bridge gaps in knowledge and experience related to health and wellness. Additionally, 59% of students (19 respondents) chose better communication between healthcare professionals and patients.
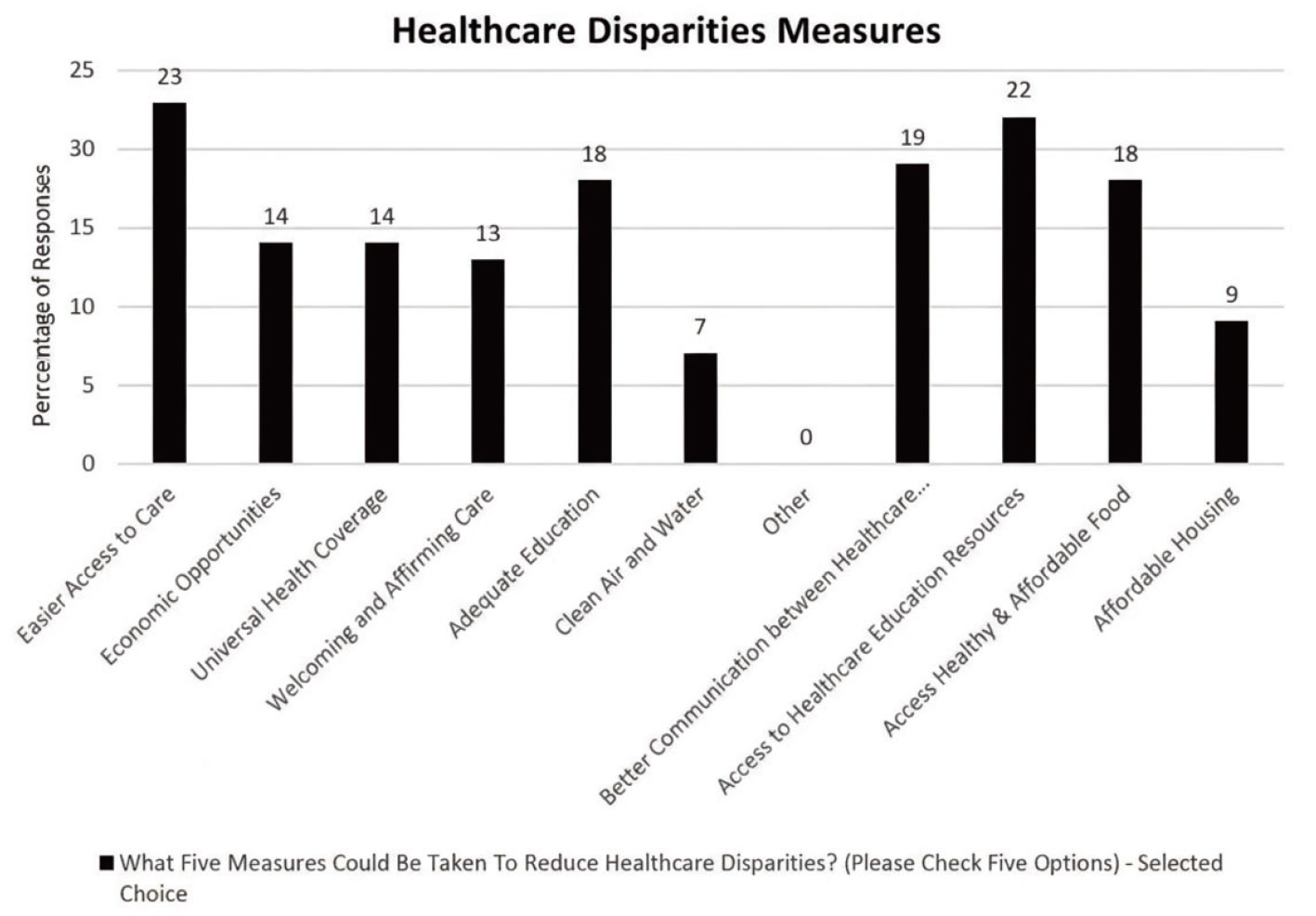
Figure 2.
Healthcare disparities measures
Also, 56% of respondents (18 individuals) noted adequate education as an essential measure, along with access to healthy and affordable food. Additional measures highlighted by fewer respondents included economic opportunities, 44% (14 respondents), universal health coverage 44% (14 respondents), ensuring welcoming and affirming care, 41% (13 respondents), and affordable housing, 28% (9 respondents). In the broader discussion on health disparities, 22% (7 respondents) emphasized the need for clean air and water. The findings illustrate a comprehensive approach among students to address healthcare disparities, emphasizing education, access, and communication as foundational measures for fostering health equity in their communities.
4.Discussion
SDOH are the conditions in which individuals are born, grow, live, work, and age, influencing health outcomes and equity.[11] Understanding SDOH is crucial for nursing students, as it enhances their ability to provide comprehensive care and advocate for policies that address healthcare disparities. Nurses are pivotal in improving health equity by influencing patient outcomes and contributing to community health initiatives.[12] Nurses are uniquely positioned to advocate for marginalized populations, including low-income families, racial and ethnic minorities, and individuals with chronic conditions.[13]
Nurses’ patient interactions enable patients to navigate complex healthcare systems and ensure access to necessary care. Research suggests that nurses can improve outcomes for underserved populations by addressing the structural factors that contribute to health disparities.[14] Nurses are trained to provide culturally sensitive care by considering patients’ social, linguistic, and cultural needs, thereby removing barriers and improving health outcomes.[15] They identify and address social, economic, and environmental factors affecting health, such as access to healthy food, safe housing, and transportation. Nurses also contribute to community health programs, such as vaccination clinics and wellness checks, helping eliminate barriers to care, including geographic isolation and a lack of transportation. Additionally, nurses are powerful advocates for health policies that address SDOH and reduce health disparities.[16]
Student nurses’ understanding of SDOH is influenced by their knowledge, attitudes, and lived experiences, like their relationships with family and peers. Community resources, including access to healthcare and socioeconomic opportunities, further shape health outcomes.[17] The SEM helps analyze how nursing education, including curricula and clinical exposure, influences students’ perceptions of health disparities and their root causes. The SEM framework emphasizes the complexity of addressing health disparities and provides insights into how future nurses can confront systemic health inequities.
The survey results indicate a strong baseline familiarity with health disparities among student nursing respondents (see Figure 1): 64% report being extremely or very familiar, 32% moderate or slight familiarity, and only 4% limited or no familiarity. Given this distribution, educational programming can move beyond introductory definitions for most learners and instead emphasize deeper, higher-order content, including structural and systemic drivers of inequity, the mechanisms by which disparities are produced and sustained, and evidence-informed strategies for clinical, community, and policy-level intervention. At the same time, respondents with moderate or slight familiarity would benefit from targeted resources, such as workshops or guided discussions, that strengthen conceptual clarity about causes, consequences, and solution pathways, including practice- and policy-based approaches. For the small subgroup with minimal familiarity, foundational instruction (i.e., core content on social determinants of health) is warranted to ensure a consistent knowledge base across the student population. Overall, the findings suggest that respondents have sufficient general awareness to support meaningful engagement, while underscoring the need for tiered learning opportunities that deepen applied understanding and ensure foundational competencies for all.
In contrast, previous studies have highlighted significant gaps in nursing students’ knowledge and understanding of SDOH.[18] Many nursing students recognize terms associated with SDOH, they often overlook the long-term impacts of factors such as poverty, education, and housing. Although students acknowledged the importance of SDOH in nursing practice, they struggled to apply this knowledge in clinical settings because SDOH was insufficiently integrated into nursing curricula.[19] In addition, nursing students had a basic understanding of SDOH but lacked the comprehensive knowledge to incorporate these concepts into patient care. A study examined that firsthand experiences and societal norms often shape students’ perceptions of SDOH, but these perceptions may not always lead to effective practice.[20] A study found that nursing students who were exposed to SDOH focused curricula and clinical experiences in underserved communities developed a deeper understanding of how these factors impact patient care. Another study highlighted that active learning strategies, such as community-based learning and case studies, promote a more holistic understanding of SDOH among nursing students.[21] Further clinical exposure and SDOH education are crucial for improving students’ competencies in addressing health disparities.
While existing literature explores nursing students’ understanding of SDOH, several areas remain underexplored. The effectiveness of cultural competence training in enhancing nursing students’ ability to address SDOH remains unclear, and further research is needed to evaluate its impact on preparedness for managing health disparities. Additionally, longitudinal studies do not yet examine how SDOH education influences clinical practice and patient outcomes over time.[22] The role of interprofessional education in teaching SDOH compared to traditional methods requires further investigation to evaluate which pedagogical practice is more effective. In addition, community-based learning might be beneficial, however, its specific impact on nursing students’ understanding and application of SDOH needs further exploration. Addressing the previously mentioned gaps in nursing didactics could lead to more effective educational strategies, better equipping nursing students to understand SDOH, and alleviating health disparities in their careers.
4.1Thematic summary of student responses on implicit bias and the IAT test
Implicit bias can contribute to healthcare disparities.[23] It is vital that educators prepare future nurses with the knowledge and skills to identify and mitigate implicit biases.[24] In exploring the concept of implicit bias, a series of student responses shed light on their familiarity with the topic and their reflections on the Implicit Association Test (IAT). The survey aimed to gauge nursing students’ familiarity with the concept of implicit bias, and the results indicated varying levels of familiarity. The data revealed a spectrum of understanding regarding implicit bias among participants. Only 2% of respondents reported being “not familiar at all,” while 5% were “slightly familiar.” In contrast, 37% identified as “very familiar” and 32% as “extremely familiar,” highlighting students’ general awareness of the concept.
Nursing students acknowledged that the test revealed biases they were previously unaware of, prompting them to reflect on their preconceived notions. Survey participants felt the outcomes aligned with their self-perceptions, while the implications of their implicit biases surprised others. For instance, one student expressed shock at discovering a slight preference for one racial group over another despite believing they approached others without prejudice. Students articulated their definitions of implicit bias, often emphasizing its subconscious nature. Descriptions included phrases like “subconscious attitudes,” “preconceived judgments,” and “unintentional prejudice.” The survey responses indicate a shared understanding that implicit bias operates below conscious awareness and can significantly influence behavior and decision-making. The responses suggest a collective desire for growth and knowledge about implicit biases, convey a commitment to confronting and mitigating them, and acknowledge that awareness is a crucial first step. The thematic analysis of these responses demonstrates that nursing students, in various capacities, are aware of their own biases. The nursing students expressed a motivation to explore their biases further, with comments emphasizing the importance of treating all individuals with fairness, irrespective of race or background.
4.2Limitations
The participants did not represent the entire student nursing population, and the assessment was conducted over one academic year. Consequently, a range of experiences were not captured within this sample. The small sample size of nursing students is a limitation, however, rich perspectives were still obtained. The IAT and the SEM were used to improve the credibility of the findings. Other limitations included students’ own biases, sociocultural beliefs, and awareness of SDOH.
5.Conclusion
This study offers valuable insights into nursing students’ understanding of the root causes of healthcare disparities through the SEM lens. The research highlights the complexity of addressing health disparities in nursing education by examining how individual, community, and societal factors shape student perceptions of social determinants of health. The findings reveal broad awareness among student nurses of critical issues such as economic challenges, access to care, and systemic inequities. While most students reported receiving training on these topics through coursework, cultural competence programs, and clinical experiences, the depth of their understanding varied. Those with more extensive exposure, through research projects and practical experiences, demonstrated a nuanced grasp of how social factors impact healthcare outcomes. The study underscores the importance of integrating comprehensive SDOH education into nursing curricula to better prepare future nurses for addressing disparities in their practice. The emphasis on cultural competence, a core theme among participants, suggests that enhancing this aspect of training could significantly improve care delivery and reduce biases in healthcare settings.
Moreover, the results highlight the need for systemic changes, including increased access to educational resources, improved communication between healthcare providers and patients, and more inclusive approaches to care. By addressing these areas, nursing education can be pivotal in fostering a new generation of healthcare professionals equipped to tackle healthcare disparities.
The research contributes to a deeper understanding of how student nurses perceive and respond to healthcare disparities. It points to the need for ongoing education, reflection, and structural changes to address these complex issues effectively. The insights will inform future curriculum development and support efforts to build a more equitable healthcare system. The study’s findings also provide a foundation for further research on integrating and expanding SDOH training in nursing programs, ensuring that all students are prepared to advocate for health equity in their professional practice.
Authors contributions
Led by Dr. Kirk A. Johnson and Dr. Yanick Joseph, they were responsible for study design, revision, and data interpretation. Tracy Borelus was responsible for data collection. All authors read and approved the final manuscript.
Funding
This work was supported by Montclair State University’s College of Humanities and Social Sciences.
Conflicts of Interest Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Informed consent
Obtained.
Ethics approval
The Publication Ethics Committee of the Association for Health Sciences and Education. The journal’s policies adhere to the Core Practices established by the Committee on Publication Ethics (COPE).
Provenance and peer review
Not commissioned; externally double-blind peer reviewed.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Data sharing statement
No additional data are available.
Acknowledgements
We greatly appreciate the valuable contributions of Montclair State University’s Nursing program and every individual who took the time to participate in this study.
References
- Smith J. Healthcare inequities persist, creating disparities in access, quality, and outcomes across different populations. J Health Disparities. 2022;10(2):45-62.
- Artiga S, Hinton E. Beyond health care: the role of social determinants in promoting health and health equity [Internet]. 2018. https://www.kff.org/racial-equity-and-health-policy/issue-brief/beyond-health-care-the-role-of-social-determinants-in-promoting-health-and-health-equity/
- Bailey Z, Krieger N, Agénor M. Structural racism and health inequities in the USA: evidence and interventions. Lancet. 2017;389(10077):1453-63. doi:10.1016/S0140-6736(17)30569-X
- Berkman N, Sheridan S, Donahue K. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155(2):97-107. doi:10.7326/0003-4819-155-2-201107190-00005
- Greenwald A, McGhee D, Schwartz J. Measuring individual differences in implicit cognition: the implicit association test. J Pers Soc Psychol. 1998;74(6):1464-80. doi:10.1037/0022-3514.74.6.1464
- Project Implicit. Implicit Association Test [Internet]. 2024. https://implicit.harvard.edu/
- McLeroy K, Bibeau D, Steckler A. An ecological perspective on health promotion programs. Health Educ Q. 1988;15(4):351-77. doi:10.1177/109019818801500401
- Vo A, Tao Y, Li Y. The association between social determinants of health and population health outcomes: ecological analysis. JMIR Public Health Surveill. 2023;9(1):e44070. doi:10.2196/44070
- Sagi D, Rudolf M, Spitzer S. A social-ecological approach to promote learning health disparities in the clinical years: impact of a home-visiting educational program for medical students. BMC Med Educ. 2022;22:698. doi:10.1186/s12909-022-03755-3
- Baron S, Beard S, Davis L. Promoting integrated approaches to reducing health inequities among low income workers: applying a social-ecological framework. Am J Ind Med. 2014;57(5):539-56. doi:10.1002/ajim.22174
- World Health Organization. Social determinants of health [Internet]. 2020. https://www.who.int/social_determinants/en/
- Hassmiller S, Wakefield M. Nurses’ role in advancing health equity. Am J Nurs. 2022;122(3):28-33.
- Williamson L. Nurses as advocates for marginalized populations. J Nurs Scholarsh. 2024;56(2):116-23.
- Williams A, Omokhodion F, Allen D. Social determinants of health in nursing practice: a scoping review. Public Health Nurs. 2021;38(4):572-82.
- Fabry J, McDermott T, Wilford M. Culturally sensitive nursing care: addressing social determinants of health. J Nurs Educ. 2024;63(3):132-9.
- Thornton P, Persaud R. Nursing students’ awareness of social determinants of health: a preliminary study. Nurs Educ Perspect. 2018;39(2):106-9.
- Hudson M. Community resources and health outcomes: a nursing perspective. J Community Health Nurs. 2024;41(1):42-8.
- Lee S, Willson P. Addressing social determinants of health in nursing education: the need for a comprehensive approach. J Nurs Educ. 2020;59(8):467-74.
- McQueen L, Cockrell D, LaGrone S. Preparing nursing students to address social determinants of health in clinical practice: a qualitative study. J Nurs Educ. 2020;59(6):321-6.
- Bartholomew M, Bentley G, Taylor C. Understanding nursing students’ perspectives on social determinants of health: a mixed-methods study. Nurse Educ Today. 2020;94:104579.
- Harrison M, Jones L, King L. Incorporating social determinants of health into nursing curricula: the case for active learning. Nurs Educ Perspect. 2019;40(5):292-5.
- Hamilton J, Swan B, McCauley L. Integrating a social determinants of health framework into nursing education. 2023:9-53. editors doi:10.1007/978-3-031-21347-2_2
- Lopez L. Implicit bias: more than a buzzword. Am Nurse J. 2024;19(11):24-8. doi:10.51256/ANJ112424
- Bartley T, O’Connor R, Beard K. Should all nurses be required to complete implicit bias training?. Am J Nurs. 2023;123(11):20-1. doi:10.1097/01.NAJ.0000995336.31551.4e
 This work is licensed under a
This work is licensed under a 