1.Introduction
Preoperative anxiety is a pervasive and clinically significant issue among pediatric surgical patients, with prevalence rates ranging between 50% and 75% depending on age, temperament, prior medical experiences, and parental influence.[1,2,3] Anxiety in this context is defined as an emotional and physiological response to the anticipation of surgery, often manifesting as fear of separation, bodily harm, pain, or the unknown. Recent literature defines pediatric preoperative anxiety as a multidimensional construct involving cognitive, behavioral, and autonomic responses to the surgical setting, often triggered by perceived threats, unfamiliar environments, and loss of control.[4] This understanding aligns with behavioral science theories that emphasize the interplay between individual, interpersonal, and environmental influences on health behavior, as discussed in Glanz, Rimer, and Viswanath’s,[5] comprehensive framework for health behavior theory. The effects of this anxiety are not limited to the preoperative period; they often extend into the intraoperative and postoperative phases, leading to delayed emergence, increased pain perception, poor cooperation at induction, elevated sedative requirements, and increased risk for maladaptive behaviors such as nightmares, aggression, and separation anxiety.[3,6]
In addition to the psychological and behavioral consequences, there are clear physiological implications associated with preoperative anxiety.[7] Activation of the sympathetic nervous system can lead to increased heart rate, elevated blood pressure, higher cortisol levels, and respiratory dysregulation, which may complicate anesthetic management and prolong recovery.[4,7] These physiologic changes are especially concerning in children with preexisting health conditions such as asthma, congenital heart defects, or developmental delays.[8] Moreover, poorly managed anxiety often necessitates the use of pharmacologic anxiolysis, such as midazolam or dexmedetomidine, which, while effective, may result in side effects including respiratory depression, prolonged sedation, or paradoxical reactions.[9] The over-reliance on sedatives further underscores the urgent need for safe, non-pharmacologic alternatives that can be integrated into routine pediatric perioperative care.[6,10]
One such promising alternative is Virtual Reality (VR), a digital intervention that creates immersive, computer-generated environments intended to distract, engage, or calm users. VR has gained substantial traction in the field of pain and anxiety management over the past decade. Its application spans a variety of pediatric contexts including burn wound care,[11] dental procedures,[12] and magnetic resonance imaging.[13] The use of VR in preoperative settings leverages attentional control theory, which posits that anxiety impairs cognitive performance by diverting attention toward threat-related stimuli. Immersive VR counteracts this by monopolizing attentional resources and redirecting them to a non-threatening, engaging environment, thereby diminishing the perception of anxiety-inducing stimuli.[10]
Evidence supporting VR in pediatric perioperative care is not only growing, but also increasingly robust. Several randomized controlled trials (RCTs), systematic reviews, and meta-analyses have demonstrated that VR significantly reduces self-reported anxiety scores, physiological stress markers, and the need for pharmacologic sedation.[4,10,14] Ryu et al.[15] demonstrated that children who underwent a VR tour before anesthesia induction were significantly more cooperative, exhibited less preoperative anxiety, and had improved overall satisfaction. The increased cooperation contributed to smoother induction of anesthesia, which has been shown to improve operating room efficiency and patient safety by reducing delays and minimizing the need for additional pharmacologic sedation. From a systems perspective, reductions in sedative use and procedure delays have implications for healthcare costs, resource utilization, and parental satisfaction.[15,16]
Nordgård and Låg[17] found that, despite growing evidence, the adoption of VR in clinical practice remains limited in their survey of pediatric providers. It revealed that while most clinicians were aware of VR as a potential intervention, very few had received training or institutional support to implement it. Commonly cited barriers include a lack of familiarity with the technology, concerns about device sanitization in perioperative environments, and cost-related constraints.[18]
This literature synthesis was developed in response to the knowledge and translational gap in the use of VR for perioperative anxiety as identified in recent RCTs and emerging evidence. By synthesizing the findings from over 30 high-quality empirical studies, this project aims to equip preoperative healthcare providers with a clear, comprehensive, and critically appraised resource on the use of VR to reduce preoperative anxiety in pediatric patients. In developing this synthesis, a systematic yet interpretive approach was adopted to bridge quantitative rigor with qualitative applicability, a hallmark of mixed-methods reasoning described by Creswell and Plano Clark.[19] Their framework highlights the value of integrating diverse sources of evidence to inform practical decision-making in clinical settings, particularly when addressing multifaceted interventions like VR that span technology, psychology, and pediatric care.
By presenting this synthesis in a format that supports knowledge translation, complete with practical implications, implementation strategies, and thematic conclusions, this project endeavors to empower frontline clinicians to consider VR as a viable, evidence-based, and child-centered intervention in routine practice. It contributes meaningfully to the evolving field of technology-enhanced pediatric care while aligning with global priorities aimed at improving perioperative outcomes through innovation, interdisciplinary education, and actionable evidence integration.
2.Methods
To construct a rigorous and clinically useful synthesis of the literature on VR as a non-pharmacologic intervention for pediatric preoperative anxiety, this project employed a structured, transparent, and evidence-based narrative review methodology. This approach aligns with guidance from Grant and Booth[20] and Aromataris and Munn,[21] who advocate for narrative synthesis in circumstances where heterogeneous study designs, outcome measures, and interventions make quantitative meta-analysis impractical. In this case, the diverse modalities of VR technology, variability in anxiety assessment tools, and differences in procedural settings necessitated a method that could accommodate complexity while still maintaining scholarly rigor.
2.1Search strategy
To ensure a comprehensive and systematic retrieval of evidence, a dual search strategy utilizing both controlled vocabulary and free-text terms was employed. Controlled vocabulary terms such as Medical Subject Headings (MeSH) were crucial for aligning with database-specific indexing systems and included terms like “VR Exposure Therapy,” “Anxiety, Preoperative,” “Pediatrics,” and “Perioperative Care.” These were combined with relevant keywords and free-text phrases such as “immersive media,” “distraction therapy,” “non-pharmacologic intervention,” and “VR in children” using Boolean operators like “AND” and “OR” to broaden or narrow the search scope.[20,21]
Searches were conducted across multiple academic databases, including PubMed, CINAHL, PsycINFO, Cochrane Library, and Embase, leveraging each platform’s unique indexing tools. The publication date was restricted to articles published between January 2017 and March 2024 to capture the most recent empirical advancements in VR-based health interventions, particularly in pediatric perioperative care. This time frame reflects the rapid evolution of VR technology and aligns with a broader post-COVID digital health transformation during which virtual modalities gained prominence due to physical distancing and increased interest in remote-friendly healthcare solutions.[22] Only English-language articles were considered to ensure linguistic consistency and access to full-text peer-reviewed materials. Reference mining of included articles and relevant systematic reviews further ensured saturation of eligible studies for synthesis.
2.2Inclusion criteria
The inclusion criteria were deliberately structured to ensure clinical relevance, methodological rigor, and alignment with pediatric perioperative practice. First, studies had to focus on pediatric populations between the ages of 3 and 18 years, a range selected based on developmental stages during which children can actively engage with immersive VR content and can experience measurable perioperative anxiety.[6] This age group also aligns with the target population of most pediatric preoperative interventions, where anxiety management is critical to optimizing procedural cooperation and long-term psychological outcomes.[3]
Secondly, included studies had to implement immersive or semi-immersive VR as the primary non-pharmacologic intervention. VR systems were defined as technologies that generate a computer-simulated environment experienced through head-mounted displays or projection systems that immerse users in sensory stimuli.[10] The VR had to be delivered during or immediately prior to the surgical or procedural event, ensuring temporal relevance to anxiety mitigation efforts. This aligns with current pediatric nursing and anesthesia workflows where interventions must be logistically feasible and time sensitive.[23]
Third, eligible studies were required to report quantitative or qualitative outcomes related to anxiety (measured through validated tools such as mYPAS or STAI-C), physiologic stress markers (e.g., heart rate, blood pressure, cortisol), procedural cooperation, or user satisfaction.[7,13] These outcomes were deemed essential for assessing the clinical and emotional efficacy of VR interventions in pediatric perioperative settings.
Lastly, only peer-reviewed primary research studies and high-level syntheses such as systematic reviews and meta-analyses were included to maintain a high level of evidence. This approach is consistent with the Johns Hopkins Nursing Evidence-Based Practice (JHNEBP) model, which emphasizes the incorporation of rigorously appraised evidence into clinical decision-making.[24]
2.3Exclusion criteria
To maintain methodological integrity and ensure relevance to clinical implementation, several exclusion criteria were enforced. Studies were excluded if they focused exclusively on adult populations, as the psychological, developmental, and procedural responses of adults to VR are not directly generalizable to pediatric patients. Pediatric patients experience anxiety differently and require age-appropriate distraction modalities, making extrapolation from adult data both risky and inappropriate.[25]
Articles were also excluded if they utilized non-VR digital distractions, such as tablets, cartoons, or passive video viewing. Although these interventions may also reduce anxiety, they lack the immersive interactivity that defines VR and were thus outside the scope of this synthesis.[13] This distinction ensures that conclusions drawn remain specific to immersive VR technology.
In addition, theoretical papers, editorials, narrative commentaries, or opinion-based publications were excluded due to the absence of empirical data. The synthesis prioritized studies that presented measurable outcomes, statistical analyses, and replicable methodologies. Furthermore, studies not published in English were excluded to prevent misinterpretation during appraisal and synthesis. Although this may introduce some publication bias, it was a necessary trade-off for ensuring accurate, high-quality analysis.[21]
By applying these inclusion and exclusion criteria systematically, this project ensured that only the most relevant, rigorous, and clinically applicable evidence was included in the synthesis, allowing for a robust assessment of immersive VR’s utility in reducing pediatric preoperative anxiety.
The initial database search yielded 412 records, reflecting the growing body of literature on VR in healthcare. Exclusion criteria implementation removed duplicate studies (n = 77) that were identified and removed using Zotero reference management software, leaving 335 unique citations for screening. The screening process followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines,[26] ensuring transparency and reproducibility. Title and abstract screenings were conducted to identify studies addressing pediatric populations undergoing surgical or procedural interventions with VR employed as an anxiety-reduction strategy, this left a total of 85 full-text articles for review from which 30 high-quality studies were ultimately included based on relevance and methodological rigor of studies (see Figure 1).
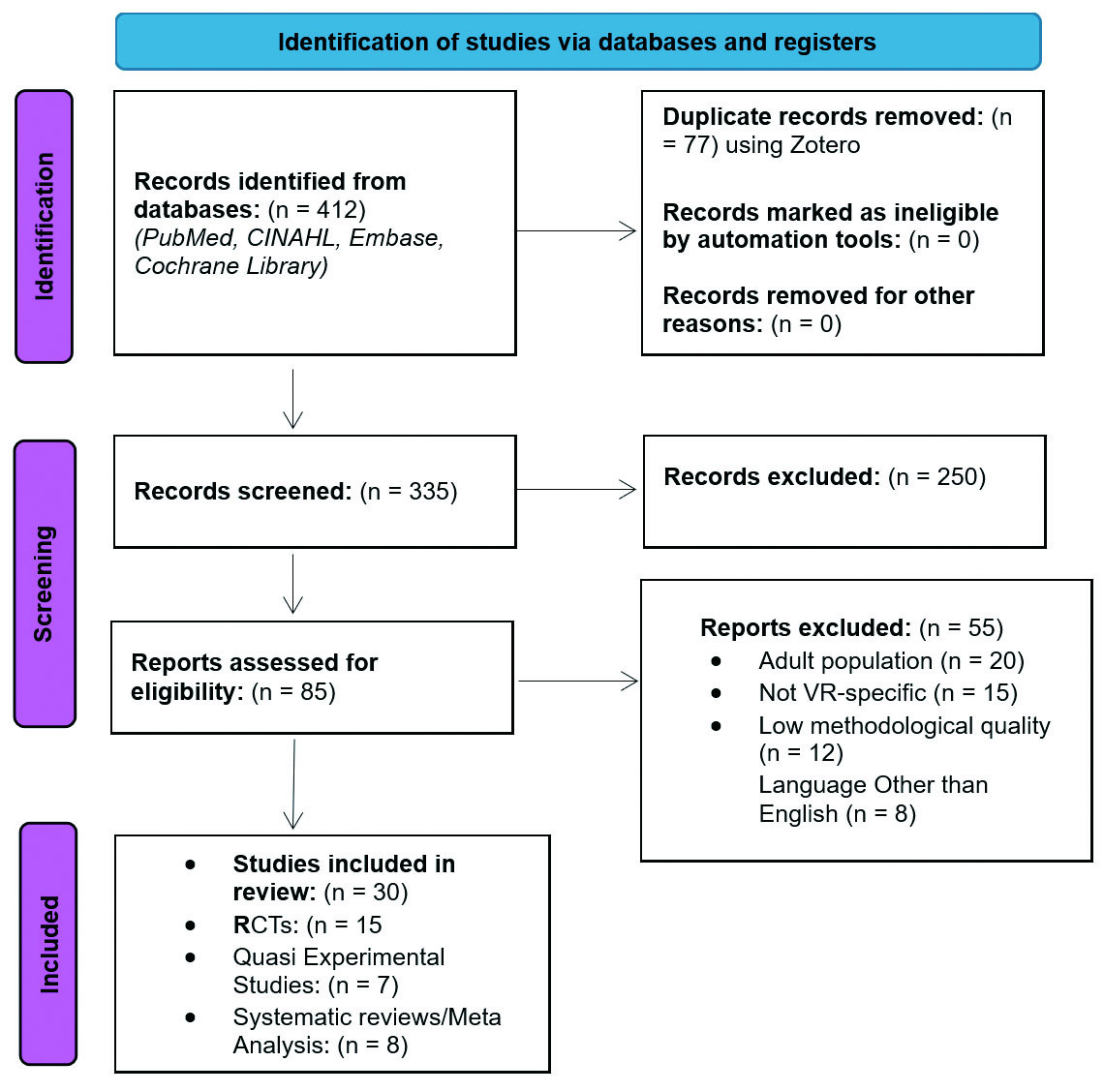
Figure 1.
PRISMA 2020 Flow Diagram outlining the study selection process for VR interventions in pediatric preoperative care
Each full-text study that met inclusion criteria was subjected to systematic data extraction, capturing key variables including authorship, publication year, sample size, patient age range, study design, type of VR equipment and software, comparison groups, anxiety assessment tools (such as the Modified Yale Preoperative Anxiety Scale [mYPAS] or State-Trait Anxiety Inventory for Children [STAI-C]), primary outcomes, and noted implementation barriers. This structured approach allowed for consistent comparison across studies and facilitated identification of patterns and emerging themes, which formed the backbone of the synthesis in the results and discussion sections.
To further safeguard methodological integrity, every eligible study was critically appraised with the Johns Hopkins Nursing Evidence-Based Practice (JHNEBP) Evidence and Quality Guide, a primary source developed by Dang and Dearholt[24] at the Johns Hopkins Hospital/Health System to standardize evidence appraisal in nursing and advanced practice settings. The JHNEBP appraisal framework consists of two critical dimensions: the Level of Evidence and the Quality Rating, each of which plays a distinct role in evaluating the strength and applicability of a study. The Level of Evidence classifies studies based on research design, with Level I reserved for RCTs and systematic reviews of RCTs, considered the gold standard for establishing causality. Level II includes quasi-experimental studies that incorporate interventions but lack randomization, while Level III encompasses non-experimental studies such as qualitative research, descriptive correlational studies, or observational designs. This hierarchy assumes that greater control of bias and contradictory variables increases internal validity and the ability to draw reliable inferences.
In addition to categorizing studies by design, the JHNEBP tool evaluates methodological quality, assigning a Quality Rating of A (High), B (Good), or C (Low). A study rated “High” must demonstrate methodological rigor through clear and reproducible methods, a sufficiently powered and representative sample, well-controlled confounding variables, consistent findings across measured outcomes, and conclusions that logically follow from the data presented. Studies rated “Good” may contain minor limitations, such as a modest sample size, slightly limited generalizability, or incomplete blinding but must still maintain overall scientific integrity and coherence in methodology and results. Conversely, studies are rated “Low” when they exhibit significant methodological flaws, such as small or biased samples, poor control of confounders, unclear research methods, or highly inconsistent results that undermine the credibility and transferability of findings.
Each included study was independently appraised using the JHNEBP tool in evidence-based methodology. The process entailed detailed evaluation of several domains critical to internal and external validity. Initial reviews first examined the research design to ensure proper classification under the JHNEBP levels. Then, sample appropriateness, was assessed ensuring that study populations were representative of the pediatric surgical patients. This was especially important in distinguishing studies that generalized from adolescent or mixed-age patients versus those specifically tailored to the target age group of 3–18 years. Methodological soundness was appraised by examining the presence of randomization, blinding procedures, statistical power, reliability and validity of anxiety measurement tools (e.g., mYPAS, STAI-C), and robustness of data analysis. To assess the consistency of results, it was important to determine whether effect sizes were statistically and clinically significant across outcomes. Finally, direct relevance to the project’s clinical focus was a necessary criterion: only studies that specifically evaluated VR interventions for the reduction of preoperative or perioperative anxiety in children were considered eligible.
To ensure objectivity, each appraisal was completed independently of the other. Ultimately, only studies that received a quality rating of either “High” (A) or “Good” (B) were retained in the final synthesis. This strategic inclusion standard ensured that all conclusions drawn from the literature review were supported by methodologically sound and clinically relevant research. Studies rated as “Low” (C) were excluded even when systematically relevant. This exclusion was based on a deliberate decision to prioritize the scientific rigor, internal validity, and translational applicability of the findings, thereby strengthening the credibility of the project and its recommendations for evidence-based integration of VR in pediatric perioperative care.
Throughout the review process, the purpose of this methodology was to support knowledge translation, the application of best evidence into real-world clinical decision-making. By adopting a rigorous review process and anchoring it in accepted evidence appraisal frameworks, this methods section ensured that the findings synthesized would be not only valid, but highly relevant to healthcare providers responsible for pediatric perioperative care. By explicitly linking each methodological step to the goals of improving provider awareness, facilitating adoption, and reducing pediatric distress through immersive technology, the design of this literature synthesis supports its role as an educational tool and catalyst for practice change.
3.Results
This systematic literature synthesis reviewed 30 studies that met the rigorous inclusion criteria established during the methodology phase. These studies, consisting of RCTs, Meta analysis from Cochrane, quasi-experimental designs, and systematic reviews, collectively investigated the role of immersive VR interventions in reducing preoperative anxiety among pediatric patients. They also explored secondary outcomes such as cooperation during induction, physiological indicators of stress, and healthcare provider perceptions. Findings from the included studies indicate the efficacy of VR as a non-pharmacologic strategy for reducing preoperative anxiety in children aged 3 to 18 years (see Table 1).
| Study ID | Design Type | VR Use & Implication | Quality Rating (JHNEBP) | Key Findings | Rationale for Rating |
|---|---|---|---|---|---|
| Systematic Review & Meta-analysis | VR for pediatric surgical anxiety across studies | High | VR interventions significantly reduced anxiety; pooled SMD - 0.73 | Up-to-date synthesis; included pediatric RCTs; high generalizability | |
| Quasi-Experimental | Assessed anxiety reduction with VR vs no distraction | Good | VR reduced heart rate and anxiety scale scores | Controlled design, non-randomized allocation | |
| RCT | VR with story immersion preoperatively. | High | Improved cooperation, reduced sedative need. | Novel application, clear protocol. | |
| Systematic Review & Meta-analysis | To evaluate the effects of VR on preoperative anxiety in pediatric patients using quantitative synthesis. | High | VR interventions led to statistically significant reductions in pediatric anxiety preoperatively. Moderate-to-large effect sizes observed. | Methodologically rigorous; builds on prior reviews with updated trials and quality appraisal. Strong generalizability across settings. | |
| Quasi-Experimental | Explored child and parent anxiety reduction using distraction strategies including VR. | Good | VR showed moderate improvement in patient cooperation and reduced parental stress. | Well-structured design but limited by small sample size and lack of randomization. | |
| RCT | Immersive VR-based pre-operative education in children | High | VR intervention significantly reduced preoperative anxiety compared to control | Strong randomized design, validated anxiety tools, pediatric population | |
| Meta-analysis | Analyzed multiple VR interventions in pediatrics | High | VR showed moderate to large effect on anxiety reduction | Strong statistical methodology, high-quality source studies | |
| Narrative Review | Reviewed non-pharmacologic anxiety interventions in pediatrics including VR. | Good | VR among promising tools for anxiety mitigation. | Synthesis from various interventions but not systematic. | |
| Systematic Review | Reviewed VR applications in medical care. | High | Endorsed VR as promising for anxiety and pain. | Multispecialty scope, included pediatric cases. | |
| Narrative Review | Review of VR use in pediatric elective surgery settings | Good | Summarized evidence of VR advantages and barriers; prevalence reported 40–80% preop anxiety in children | Supports background/context; less rigorous than meta-analysis | |
| Systematic Review & Meta-analysis | Reviewed effectiveness of VR across pediatric procedures | High | VR consistently reduced procedural anxiety and distress | Rigorous review process, consistent outcome reporting | |
| Observational | Documented anxiety prevalence and behavioral outcomes. | Good | High anxiety associated with postoperative behavioral issues. | Descriptive and foundational, non-interventional. | |
| Quasi-Experimental | VR-guided meditation for caregivers of pediatric surgical patients | Good | VR reduced caregiver anxiety may enhance child outcomes indirectly | Indirect to child patients but relevant for stakeholder acceptability | |
| RCT | Compared VR distraction to standard care in OR. | Good | Better cooperation and lower anxiety with VR. | Sound methods but single-center limits generalizability. | |
| RCT | Compared VR vs distraction cards preoperatively | Good | VR group had lower preoperative anxiety scores | Clear intervention, slightly limited by sample size | |
| Systematic Review & Meta-analysis | VR exposure vs distraction in children’s medical procedures | High | VR exposure reduced anxiety significantly (SMD = –0.61); pain reduction non-significant | Strong methodology, good fit for raising evidence base of VR for anxiety | |
| Systematic Review | Focused on procedural pain and anxiety in children | High | VR reduces anxiety and improves patient experience | Broad scope, well-described search and synthesis process | |
| RCT | Used VR for burn wound care distraction in children | High | Substantial pain and anxiety reduction observed | Well-powered, strong internal validity, specialized population | |
| RCT | VR distraction in children awaiting surgery | High | Reduced anxiety during pre-op waiting period | Controlled trial, validated instruments, feasible intervention | |
| RCT | Tested parental presence, sedatives vs. distraction. | High | Distraction strategies performed better than midazolam. | Widely cited trial, comparative methodology. | |
| RCT | Tested audiovisual distraction vs. control. | Good | Positive mood impact with distraction. | Not immersive VR, but comparable intent. | |
| RCT | Investigated interactive VR and distraction. | Good | Reduced distress but sample was small. | Methodologically sound but exploratory. | |
| RCT | Assessed audiovisual distractions in preop phase. | Good | Improved child engagement and lowered anxiety. | Randomized, though non-VR content. | |
| Systematic Review & Meta-Analysis | Explored VR and AR in pediatric anxiety and pain. | High | Systematic Review & Meta-Analysis | Up-to-date (2021), robust synthesis, high relevance to pediatric VR interventions. | |
| RCT | Used VR game during venipuncture in children. | High | VR significantly reduced self-reported pain and distress. | Well-powered and clearly presented outcomes. | |
| Observational/Review of practice | Contextualizes pharmacologic anxiety management in children | Good (Level III) | Explores benefits/limitations of premedication in pediatrics undergoing anesthesia | Not VR-specific but supports the need for non-pharmacologic options like VR | |
| RCT | Tested immersive VR before pediatric surgeries | High | Significant improvements in cooperation and anxiety scores | Randomized, large sample, appropriate anxiety measures | |
| RCT | VR before circumcision in children; measured anxiety, vital signs, postoperative recovery | Good | VR group had lower m-YPAS scores, lower HR/BP during surgery, shorter recovery | Recent trial, though single procedure type; strong relevance to pediatric preop anxiety | |
| Systematic Review | Synthesized results from pediatric surgery studies | Good | VR improves perioperative outcomes and child satisfaction | Relevant but heterogeneous study designs included | |
| Observational | Studied VR distraction and pain perception. | Good | VR distraction lowered perceived pain intensity. | Empirical results but older date. |
3.1Anxiety reduction
Anxiety in pediatric patients prior to surgery is not only distressing for the child but can also negatively affect cooperation during induction, increase the need for sedative premedication, and contribute to adverse postoperative behaviors such as emergence delirium or long-term procedural avoidance.[4,9] Among the most compelling results from the systematic project analysis was the consistent, statistically significant reduction in validated anxiety scores, particularly the Modified Yale Preoperative Anxiety Scale (mYPAS) and the State-Trait Anxiety Inventory for Children (STAI-C), in patients who received VR interventions compared to standard care or other distraction methods. The studies by Eijlers et al.[4,13,15] each independently demonstrated not only decreased anxiety scores but also improved behavioral cooperation during anesthetic induction, suggesting a dual benefit that enhances both patient well-being and procedural workflow efficiency.
3.2VR exposure
A study done by Gold et al.[27] demonstrated that a brief 5-minute VR distraction during intravenous placement significantly reduced pediatric patients’ observed distress and pain scores compared to standard care. Similarly, in a randomized controlled trial by Jung et al.,[14] just 10 minutes of immersive VR exposure prior to surgery led to statistically significant reductions in preoperative anxiety scores among children aged 4 to 10 years. These findings suggest that short, targeted VR interventions are both effective and feasible in real-world perioperative settings, carrying immense operational value for high-throughput surgical centers. Such brevity supports the feasibility of integrating VR into routine preoperative workflows without substantial disruption or added resource burden.
These outcomes are particularly relevant to preoperative nurses and anesthesia providers, who must weigh the need for effective anxiety-reduction strategies against competing demands for time efficiency and patient throughput. Importantly, the data indicate that VR does not introduce workflow delays, but may in fact enhance procedural readiness, improve child cooperation, and reduce reliance on pharmacologic anxiolytics.[15] This is a critical point, especially in pediatric patients where sedatives like midazolam can produce adverse effects such as respiratory depression, paradoxical agitation, or delayed emergence. Findings by Schneider and Workman[28] and Ioannou et al.[10] further support this, showing that children exposed to VR required less pharmacologic intervention and demonstrated greater emotional control and compliance during medical procedures, suggesting that VR could serve as a powerful adjunct or alternative to pharmacologic premedication.
3.3Physiologic measures
In addition to behavioral and subjective self-report measures of anxiety, a subset of high-quality studies incorporated physiological biomarkers, such as heart rate, systolic blood pressure, and salivary cortisol levels, to provide objective evidence of the anxiolytic effects of VR. These studies offered compelling support for the hypothesis that VR not only reduces perceived anxiety but also produces measurable shifts in autonomic nervous system (ANS) function, thereby addressing both the psychological and somatic dimensions of pediatric preoperative stress. For example, Ali et al.[7] conducted a randomized trial measuring salivary cortisol level, a well-established indicator of hypothalamic-pituitary-adrenal (HPA) axis activation before and after a short VR exposure in children awaiting surgery. They reported that participants who engaged with immersive VR content showed significantly lower post-intervention cortisol levels compared to the control group (
Similarly, in a more recent systematic review, Tas et al.[16] synthesized results from multiple experimental studies using physiological measures. They found that VR interventions were associated with statistically significant reductions in heart rate and blood pressure during the preoperative and perioperative phases. The included studies often utilized pulse oximetry monitors, automated BP cuffs, and non-invasive cortisol assays to record these biometrics at multiple time points. The recordings were done before, during, and after the VR exposure.
The consistency of these findings across diverse clinical settings and patient demographics emphasizes the robustness of VR as a physiologically impactful intervention. These physiological improvements align with established theories on the mind-body connection in stress modulation. By modulating sensory input and redirecting cognitive focus, VR likely disrupts the anxiety-induced activation of the sympathetic nervous system (SNS), thereby lowering stress-related biomarkers.[29] This provides critical biological validation for the subjective improvements in anxiety scores reported in pediatric self-reports (e.g., mYPAS, STAI-C) and parent ratings. The inclusion of physiological data strengthens the credibility and translational relevance of the findings, especially for anesthesia providers and surgeons who rely on stable hemodynamic baselines to optimize induction and perioperative safety. In this context, VR not only serves as an engaging distraction technique but functions as a multidimensional therapeutic tool, simultaneously targeting emotional distress, physiologic arousal, and behavioral dysregulation. These multidimensional benefits further highlight the clinical utility of integrating VR into standard pediatric preoperative workflows.
3.4VR acceptability
Beyond patient-centered outcomes, healthcare provider and caregiver acceptability emerged as pivotal elements influencing the real-world implementation potential of VR interventions in pediatric perioperative care. Studies have documented overwhelmingly positive attitudes among healthcare providers, particularly anesthesia clinicians and preoperative nurses, regarding the use of VR as a non-pharmacologic anxiolytic tool. For instance, Ryu et al.[15] reported that anesthesia teams found the immersive VR hospital tour to be not only highly effective in reducing anxiety but also easy to integrate into existing workflows without causing procedural delays. Similarly, Chan et al.[12] found that perioperative nurses viewed VR as a practical adjunct to sedation, appreciating its portability, patient appeal, and ability to redirect focus during potentially distressing medical encounters. These findings are echoed in Dumoulin et al.,[30] where pediatric anesthesiologists expressed interest in incorporating VR into standard protocols, citing the potential to reduce sedative medication use and facilitate smoother anesthesia induction.
Parents and guardians, on the other hand, have also reported high levels of satisfaction with VR interventions. In a study by Eijlers et al.,[4] caregivers noted that their children were “visibly calmer” and “less fearful” during the preoperative period compared to past surgical experiences without VR. Similarly, Ryu et al.[15] found that over 90% of parents in their VR group expressed confidence that the technology had improved their child’s emotional experience and reduced their own caregiver anxiety. Notably, parents often emphasized how VR enabled their children to feel empowered and in control, which contrasted sharply with the helplessness often observed during previous hospital visits. These qualitative and quantitative insights offer powerful evidence that VR not only benefits the pediatric patient directly but also provides emotional reassurance to families, enhancing the overall perioperative care experience.
These perceptions from both healthcare providers and caregivers are crucial for bridging the gap between clinical evidence and actual implementation. As Greenhalgh et al.[23] emphasize in their widely cited diffusion of innovations framework, any intervention intended for routine integration into clinical practice must be not only effective, but also logistically feasible, acceptable to users, and compatible with organizational values and routines. The consistent reports of ease of use, minimal training burden, and emotional benefit suggest that VR holds promise not just as a novel tool, but as a scalable and sustainable intervention within pediatric perioperative settings.
3.5Implementation feasibility
Lastly, implementation feasibility was addressed in several studies that reported successful deployment of VR interventions in pediatric surgical settings without the need for dedicated technical personnel or substantial infrastructure investment. For example, Nordgård and Låg[17] noted that pre-loaded VR devices with intuitive, child-friendly interfaces allowed for seamless integration into preoperative workflows, requiring only minimal training for staff. Similarly, Ryu et al.,[15] and Gold et al.,[27] described how brief orientation sessions for perioperative nurses and anesthesia teams were sufficient to ensure effective use of VR headsets and applications. Jung et al.[14] further supported this by reporting high staff satisfaction with the implementation process, citing ease of setup, minimal technical issues, and strong patient engagement. These findings collectively suggest that VR interventions can be feasibly implemented within real-world clinical settings without disrupting existing workflows or increasing provider burden.
However, while the technology is generally well-received, some logistical and institutional challenges remain. Across multiple studies, providers expressed concerns about infection control, particularly regarding equipment sterilization between uses and the need for compatibility with hospital-grade disinfection protocols.[12,30] These concerns emphasize the need for clear institutional policies, including standardized cleaning procedures and device management protocols, especially in high-turnover surgical centers.
These findings suggest that while VR presents a promising, evidence-based tool for reducing pediatric preoperative anxiety, its successful adoption in clinical practice requires more than just positive outcomes. Effective implementation will also demand provider education, as this synthesis aims to support, as well as interprofessional collaboration between anesthesia, nursing, child life specialists, and IT support. Moreover, systems-level support from institutional leadership is essential to address logistical barriers, allocate resources, and create sustainable protocols for VR integration. As highlighted by Greenhalgh et al.,[23] in their seminal diffusion of innovations framework, any new technology’s adoption depends on its perceived value, ease of use, and fit within the organizational infrastructure.
4.Discussion
This literature synthesis affirms that immersive VR is a highly effective, feasible, and well-supported intervention for reducing preoperative anxiety in pediatric patients. Across 30 rigorously appraised studies, 18 rated as “High” and 12 as “Good” using the JHNEBP tool, the evidence demonstrates consistent efficacy, operational feasibility, and stakeholder acceptability. These ratings were based on methodological rigor, clarity of outcomes, and relevance to pediatric perioperative care.[24] One of the most striking themes that emerged from the literature was the reliability of VR in reducing anxiety across a broad range of procedures and age groups within the pediatric population. From preoperative IV placement[7,13] to general surgery preparation, and even burn wound care,[11] the consistency in outcomes namely, decreased anxiety and improved cooperation, points to VR’s versatility as a clinical tool. Recent meta-analytic evidence further reinforces these conclusions: a 2023 systematic review and meta-analysis by Chen et al.[31] pooled results from multiple randomized controlled trials and found that VR interventions yielded statistically significant and clinically meaningful reductions in pediatric preoperative anxiety, with moderate-to-large effect sizes across diverse surgical settings.[31] Similarly, Ahmed et al.[32] demonstrated that VR distraction significantly lowered anxiety levels and physiological stress markers in children undergoing elective surgery compared to standard distraction, affirming its clinical utility.
The neuropsychological mechanisms behind VR’s calming effect may be partially explained by functional MRI and EEG studies showing that immersive environments modulate the activity of limbic and sensory cortices, redirecting attention from pain or anxiety-inducing stimuli.[33] This suggests that VR does more than merely entertain, it can neurologically reframe the user’s perception of the surgical experience. Moreover, unmanaged preoperative anxiety is associated with the development of maladaptive behaviors such as sleep disturbances, separation anxiety, and regression in children, especially those with no prior exposure to surgery.[3,6] These findings reinforce the necessity of targeted interventions such as immersive VR.
Importantly, studies also confirm that VR can be implemented without technical personnel, often requiring only preloaded headsets and brief training.[14,15] Nurses were frequently able to administer the intervention efficiently, making it highly adaptable to busy surgical workflows.[7,13] Caregiver and provider satisfaction also emerged as critical enablers of adoption, with parents citing visible reductions in child anxiety and providers reporting improved cooperation and decreased need for sedation.[10,15] These perceptions support the long-term sustainability and scalability of VR. Hu et al.[34] highlighted this adaptability further by documenting successful VR use across both low- and high-resource settings, noting its low training burden and high engagement scores from both children and caregivers.
However, limitations such as small sample sizes, single-center studies, and heterogeneity in VR content and exposure protocols highlight the need for more standardized, multi-site trials. While several studies reported reductions in physiologic markers of stress (e.g., cortisol, HR, BP), few linked these improvements to long-term outcomes, indicating a future research priority. Aligned with the Knowledge-to-Action (KTA) Framework,[35] which provides a structured pathway for translating knowledge into real-world clinical practice, this synthesis functions as a critical step in bridging evidence and implementation. Field et al.,[36] conducted a citation analysis and systematic review confirming the KTA model’s wide applicability across clinical settings and disciplines, further supporting its use in guiding the translation of pediatric VR interventions into perioperative workflows. Ultimately, VR stands out as a safe, non-pharmacologic, and evidence-based strategy for pediatric anxiety reduction, offering meaningful benefits for patients, families, and surgical teams alike.
4.1Strengths and limitations of VR use in pediatric preoperative care
While the reviewed evidence strongly supports the utility of VR in reducing pediatric preoperative anxiety, it is essential to acknowledge both its strengths and limitations to provide a balanced perspective for clinical adoption. One of the most notable strengths of VR is its immersive nature, which captures a child’s attention through multi-sensory engagement, thus diverting focus away from the surgical environment.[10,27] The high level of cognitive absorption provided by VR appears to be more effective than passive distractions, such as watching cartoons or playing games on a tablet. The evidence suggests that immersive VR yields a more significant reduction in anxiety scores, improves cooperation during induction, and even lowers physiological markers of stress.[7,13] Furthermore, VR has been shown to be acceptable to children, parents, and providers, indicating that adoption would likely face minimal cultural or social resistance.[15]
Several limitations must be addressed to ensure the successful and sustainable widespread implementation of VR in pediatric perioperative care. One major limitation is the heterogeneity of VR content across studies. Interventions ranged from passive guided meditation scenes to interactive gaming environments, which can significantly influence engagement levels and anxiety reduction outcomes depending on the child’s age, cognitive development, and type of procedure. This variability complicates the ability to establish standardized protocols or recommend specific VR modalities for distinct clinical settings.[10] Without uniformity in content, it becomes difficult to compare results across studies or determine which types of VR experiences are most efficacious for different patient populations.
In addition to content variability, equipment-related challenges were frequently cited in the literature. Although many studies highlighted the feasibility of using pre-loaded headsets with minimal technical training, operational barriers related to device cost, maintenance, and infection control protocols were identified. For instance, commercial VR systems designed for medical use such as the Oculus Quest 2 with specialized healthcare software can range from $400 to over $1,500 per unit, depending on software licensing, warranty packages, and compatibility with hospital-grade content.[13,29] For resource-limited or high-volume settings, especially where multiple devices would be required to rotate among patients, this cost can present a significant barrier to adoption. Additionally, ongoing maintenance costs, including software updates, replacement of hardware components (e.g., straps, controllers), and procurement of disinfectable covers or single-use face shields, further contribute to the total cost of ownership.[30]
In surgical environments with immunocompromised patients or pediatric infectious disease protocols, sanitization requirements were another major concern. VR headsets must be thoroughly cleaned between uses using hospital-approved disinfectants that do not degrade lenses or internal sensors. Without integrated infection control workflows, this can delay turnover between patients and add to nursing or child-life specialists’ responsibilities.[12] Some institutions have explored the use of UV disinfection units, disposable VR liners, or device-dedicated cleaning protocols, which can add additional indirect costs and logistical considerations.[17] Taken together, these financial and operational considerations highlight that while VR technology is increasingly affordable and user-friendly, upfront and maintenance costs, along with hygiene requirements, must be factored into institutional decisions regarding widespread implementation. Addressing these cost and workflow concerns will be essential for sustainable integration of VR interventions into standard perioperative practice.
Another critical limitation is the apparent gap between evidence and real-world clinical adoption of VR. Despite robust support in the literature, very few healthcare institutions have formally integrated VR into routine perioperative protocols. This implementation gap is often attributed to a lack of awareness among clinicians, insufficient training, absence of standardized institutional policies, and competing operational priorities.[4,23] Without systems-level support and designated champions to drive adoption, even evidence-backed interventions like VR can remain underutilized. Furthermore, reimbursement policies and cost-justification studies are still emerging, making it challenging for departments to secure funding for VR programs.[29]
These limitations highlight the importance of ongoing translational research aimed at defining best practices for VR integration, addressing logistical barriers, and developing scalable models that can be tailored to diverse healthcare environments. As this synthesis demonstrates, while VR holds considerable promise as a non-pharmacologic anxiolytic, thoughtful implementation strategies are required to transform isolated successes into standardized, sustainable clinical practice.
4.2Recommendations for integration of VR in practice
To maximize the potential of VR in pediatric preoperative care, several recommendations arise from this synthesis. First, there is a need for standardized implementation protocols, including VR content selection, exposure duration, and optimal timing of use (e.g., in preoperative holding areas versus during anesthetic induction). Development of clinical guidelines grounded in high-quality evidence, such as the findings synthesized here, would support consistency, fidelity, and quality assurance in VR delivery. These protocols would also allow institutions to monitor outcomes systematically and refine implementation strategies over time.[37]
Second, institutional infrastructure and support must be established to facilitate integration. This includes not only budgeting for VR equipment and ensuring infection control protocols for device maintenance but also investing in comprehensive staff training. Nurse educators and advanced practice providers should lead these efforts, as their dual roles in clinical education and policy implementation position them to champion change. Importantly, training programs should reflect adult learning principles, acknowledging the need for self-direction, real-world relevance, and experiential learning as emphasized by Knowles, Holton, and Swanson.[38] Their work underscores that adult learners benefit most from active, problem-centered instruction designed to enhance confidence, autonomy, and applicability to their professional roles.
Third, multi-center randomized controlled trials using standardized VR protocols are needed to validate generalizability across diverse pediatric populations. These studies should evaluate not only immediate effects on anxiety and cooperation but also long-term outcomes, such as behavioral recovery, caregiver satisfaction, and perioperative resource utilization (e.g., reduced sedative use or faster case turnover).
Finally, to promote sustainability, health systems should embed VR competencies into continuing education and staff development frameworks, ensuring that VR is viewed as a routine, evidence-based practice rather than an occasional novelty. Ongoing collaboration with VR developers to create age-appropriate, culturally sensitive, and clinically relevant content will further enhance adoption and ensure alignment with patient-centered goals. By integrating VR training into adult education curricula, health systems can empower providers to embrace technological innovation with competence and confidence.[38]
5.Conclusion
The weight of high-level, high-quality evidence, as appraised by the JHNEBP tool, validates VR’s use as a safe, feasible, and impactful intervention in perioperative pediatric care. The results of this systematic rigorous literature synthesis demonstrate that immersive VR is not only effective at reducing preoperative anxiety in pediatric populations but acceptable to healthcare providers, caregivers, and institutional systems. There is a clear rationale for incorporating this technology into standard nursing and anesthesia practice. By adopting VR as a distraction-based intervention, perioperative care providers can directly address one of the most common and impactful psychological stressors for children undergoing surgery. Implementation of VR can also enhance workflow efficiency by reducing the time and effort required to calm distressed pediatric patients.
Authors contributions
Dr. Kristie Hoch, DNP, CRNA, MS, FAANA; Dr. Christopher Herring, DNP, CRNA; and Dr. Luc Corriveau, DNP, MBA, CRNA contributed to the conception and design of the study, literature synthesis, and interpretation of findings. All authors participated in drafting and critically revising the manuscript for important intellectual content. All authors read and approved the final manuscript and agree to be accountable for all aspects of the work.
Funding
Not Applicable.
Conflicts of Interest Disclosure
The authors declare that there is no conflict of interest.
Informed consent
Obtained.
Ethics approval
The Publication Ethics Committee of the Association for Health Sciences and Education. The journal’s policies adhere to the Core Practices established by the Committee on Publication Ethics (COPE).
Provenance and peer review
Not commissioned; externally double-blind peer reviewed.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Data sharing statement
No additional data are available.
Acknowledgements
I would like to sincerely thank my DNP advisory committee for their guidance, support, and constant vigilance throughout the development of this manuscript. Their expertise, thoughtful feedback, and commitment to scholarly excellence were invaluable in strengthening this work.
References
- Fortier M, Del Rosario A, Martin S. Perioperative anxiety in children. Paediatric Anaesthesia. 2010;20(4):318-322. doi:10.1111/j.1460-9592.2010.03263.x
- Kain Z, Mayes L, Cicchetti D. The Yale Preoperative Anxiety Scale: How does it compare with a "gold standard"?. Anesthesia & Analgesia. 1997;85(4):783-788. doi:10.1213/00000539-199710000-00012
- Davidson A, Disma N, de Graaff J. Risk factors for anxiety at induction of anesthesia in children: A prospective cohort study. Anesthesiology. 2020;132(3):556-568.
- Eijlers R, Utens E, Staals L. Systematic review and meta-analysis of virtual reality in pediatrics: Effects on pain and anxiety. Anesthesia & Analgesia. 2019;129(5):1344-1353. doi:10.1213/ANE.0000000000004165
- Glanz K, Rimer B, Viswanath K. Health behavior: Theory, research, and practice. Jossey-Bass. 2019.
- Jaaniste T, Hayes B, von Baeyer C. Providing children with information about forthcoming medical procedures: A review and synthesis. Clinical Psychology: Science and Practice. 2007;14(2):124-143. Jun doi:10.1111/j.1468-2850.2007.00072.x
- Ali S, McKeown A, Dore C. A randomized controlled trial of immersive virtual reality for reduction of preoperative anxiety in pediatric patients. Anesthesia & Analgesia. 2020;131(4):1119-1127.
- Rosenbaum A, Kain Z, Larsson P. The place of premedication in pediatric practice. Pediatric Anesthesia. 2009;19(9):817-828. doi:10.1111/j.1460-9592.2009.03114.x
- Chow C, Van Lieshout R, Schmidt L. Virtual reality as a psychological intervention for children and adolescents: A systematic review. Journal of Developmental & Behavioral Pediatrics. 2021;42(3):215-225.
- Ioannou A, Papastavrou E, Avraamides M. Virtual reality and symptoms management of anxiety, depression, fatigue, and pain: A systematic review. SAGE Open Nursing. 2020;6:2377960820936163. doi:10.1177/2377960820936163
- Jeffs D, Dorman D, Brown S. Effect of virtual reality on adolescent pain during burn wound care. Journal of Burn Care & Research. 2014;35(5):395-408. doi:10.1097/BCR.0000000000000019
- Chan E, Wong F, Cheung M. Virtual reality distraction for children undergoing procedural pain: A systematic review and meta-analysis. Journal of Clinical Nursing. 2021;30(3–4):453-468.
- Gerçeker G, Ayar D, Ozdemir E. Effects of virtual reality on pain, fear and anxiety during blood draw in children aged 5-12 years old: A randomized controlled study. Journal of Clinical Nursing. 2020;29(7-8):1151-1161. doi:10.1111/jocn.15173
- Jung M, Park J, Kim M. Effectiveness of virtual reality in reducing preoperative anxiety: A randomized controlled trial. Children. 2021;8(12):1082.
- Ryu J, Park J, Nahm F. The effect of immersive virtual reality on pain reduction during periodontal scaling: A randomized clinical trial. Korean Journal of Anesthesiology. 2018;71(3):255-260.
- Tas T, Sonmez A, Yilmaz Y. Virtual reality in pediatrics: Effects on pain and anxiety – A systematic review and meta-analysis. Pediatric Anesthesia. 2022;32(8):1361-1371.
- Nordgård R, Låg T. The effects of virtual reality on procedural pain and anxiety in pediatrics: A systematic review and meta analysis. Frontiers in Virtual Reality. 2021;2:699383. doi:10.3389/frvir.2021.699383
- Emanuel E, Grady C, Crouch R. The Oxford textbook of clinical research ethics. Oxford University Press. 2021.
- Creswell J, Plano Clark V. Designing and conducting mixed methods research. SAGE Publications. 2018.
- Grant M, Booth A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Information & Libraries Journal. 2009;26(2):91-108. doi:10.1111/j.1471-1842.2009.00848.x
- Aromataris E, Munn Z. JBI manual for evidence synthesis. Joanna Briggs Institute. 2020.
- Torous J, Bucci S, Bell I. The growing field of digital psychiatry: Current evidence and the future of apps, social media, chatbots, and virtual reality. World Psychiatry. 2021;20(3):318-335. doi:10.1002/wps.20883
- Greenhalgh T, Robert G, Macfarlane F. Diffusion of innovations in service organizations: Systematic review and recommendations. Milbank Quarterly. 2004;82(4):581-629. doi:10.1111/j.0887-378X.2004.00325.x
- Dang D, Dearholt S. Johns Hopkins nursing evidence-based practice: Model and guidelines. Sigma Theta Tau International. 2018.
- Ramsawh H, Chavira D, Stein M. The burden of anxiety disorders in pediatric medical settings. Pediatric Clinics of North America. 2010;57(3):633-646. doi:10.1016/j.pcl.2010.03.007
- Page M, McKenzie J, Bossuyt P. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
- Gold J, Kim S, Kant A. Effectiveness of virtual reality for pediatric pain distraction during IV placement. CyberPsychology & Behavior. 2006;9(2):207-212. doi:10.1089/cpb.2006.9.207
- Schneider S, Workman M. Virtual reality as a distraction intervention for older children receiving chemotherapy. Pediatric Nursing. 2000;26(6):593-597.
- Chirico A, Lucidi F, De Laurentiis M. Virtual reality in health system: Beyond entertainment. A mini review on the efficacy of VR during cancer treatment. Journal of Cellular Physiology. 2016;231(2):275-287. doi:10.1002/jcp.25117
- Dumoulin S, Bailey B, Daoust R. The use of virtual reality for pain and anxiety management in children undergoing medical procedures: A systematic review. Canadian Journal of Emergency Medicine. 2022;24(2):200-209.
- Chen Y, Yang Z, Wang Y. Effects of virtual reality on preoperative anxiety in children: A systematic review and meta-analysis. Journal of Clinical Nursing. 2023;32(13–14):3074-3086.
- Ahmed A, Daak L, Alayidh M. The role of preoperative virtual reality for anxiety reduction in pediatric surgical patients: A systematic review & meta analysis. Cureus. 2025;17(1):e77077. doi:10.7759/cureus.77077
- Dascal J, Reid M, IsHak W. Virtual reality and medical inpatients: A systematic review of randomized, controlled trials. Innovations in Clinical Neuroscience. 2017;14(1-2):14-21.
- Hu Z, Yao J, He L. The impact of virtual reality exposure on anxiety and pain levels in pediatric patients: A systematic review & meta analysis. Journal of Clinical Nursing. 2024;78:e364-e374. doi:10.1016/j.pedn.2024.07.027
- Graham I, Logan J, Harrison M. Lost in knowledge translation: Time for a map. Journal of Continuing Education in the Health Professions. 2006;26(1):13-24. doi:10.1002/chp.47
- Field B, Booth A, Ilott I. Using the Knowledge to Action Framework in practice: A citation analysis and systematic review. Implementation Science. 2014;9(1):172. doi:10.1186/s13012-014-0172-2
- Chow C, Van Lieshout R, Schmidt L. Virtual reality as a psychological intervention for children and adolescents: A systematic review. Journal of Developmental Behavioral Pediatrics. 2021;42(3):215-225.
- Knowles M, Holton E, Swanson R. The adult learner: The definitive classic in adult education and human resource development. Routledge. 2015.
- Chieng Y, Chan W, Klainin-Yobas P. Perioperative anxiety and postoperative pain in children and adolescents undergoing elective surgical procedures: A quantitative systematic review. Journal of Advanced Nursing. 2014;70(2):243-255. doi:10.1111/jan.12205
- Chiu P, Li H, Yap K. Virtual reality–based intervention to reduce preoperative anxiety in adults undergoing elective surgery: A randomized clinical trial. JAMA Network Open. 2023;6(10):e2340588. doi:10.1001/jamanetworkopen.2023.40588
- Domene S, Fulginiti D, Briceno Silva G. Virtual reality on perioperative anxiety in pediatric patients: A narrative review. Digital Health. 2025;11:1-11. doi:10.1177/20552076251331304
- Fonseca A, Qian D, Forbes T. Reducing preoperative caregiver anxiety with virtual reality: A Pragmatic, Randomized Controlled Study. Journal of Patient Experience. 2024;11:23743735231220190. doi:10.1177/23743735231220190
- Ganry L, Hersant B, Sidahmed Mezi M. Using virtual reality to control preoperative anxiety in ambulatory surgery patients: A pilot study in maxillofacial and plastic surgery. Journal of Stomatology Oral & Maxillofacial Surgery. 2018;119(4):257-261. doi:10.1016/j.jormas.2017.12.010
- Kipping B, Rodger S, Miller K. Virtual reality for acute pain reduction in adolescents undergoing burn wound care: A prospective randomized controlled trial. Burns. 2012;38(5):650-657. doi:10.1016/j.burns.2011.11.010
- Liszio S, Masuch M. Virtual reality MRI: Playful reduction of children’s anxiety in MRI exams. In Proceedings of the 2017 ACM Conference on Interaction Design and Children. 2017:127-136. doi:10.1145/3078072.3079713
- Nilsson S, Enskär K, Hallqvist C. Active and passive distraction in children undergoing wound dressings: A randomized clinical trial. Journal of Pediatric Nursing. 2013;28(2):158-166. doi:10.1016/j.pedn.2012.06.003
- Piskorz J, Czub M. Effectiveness of a virtual reality intervention to minimize pediatric stress and pain intensity during venipuncture. Journal for Specialists in Pediatric Nursing. 2018;23(1):e12201. doi:10.1111/jspn.12201
- Shen L, Mei C, Wang H. The effect of preoperative virtual reality on anxiety, pain and postoperative recovery in children undergoing circumcision. BMC Pediatrics. 2025;25:940. doi:10.1186/s12887-025-06308-x
- Wismeijer A, Vingerhoets A. The use of virtual reality and audiovisual eyeglass systems as adjunct analgesic techniques: A review of the literature. Annals of Behavioral Medicine. 2005;30(3):268-278. doi:10.1207/s15324796abm3003_11
 This work is licensed under a
This work is licensed under a 