1.Introduction
Internationally educated healthcare providers (IEHPs) have long been part of the Canadian healthcare workforce with the highest number of registered nurses entering the country between 2019 and 2023.[1] Currently, Internationally Educated Nurses (IENs) make up about 9% of the nursing workforce[2] but remain an untapped resource that could bolster the workforce and provide culturally appropriate care to Canadians.[3]
Recruitment of IENs though is becoming more competitive. To address the nursing shortage and the threat to the sustainability of the rural healthcare workforce,[4] in 2023, Alberta Health Services (AHS, AHS is the largest healthcare provided in the province.) launched a recruitment campaign to attract IEN applicants. The College of Registered Nurses of Alberta (CRNA, CRNA is the regulatory body for licensed nurses in Alberta.) reduced barriers to entering the workforce by streamlining the transition and integration of IENs with issuing provisional permits.[5] AHS then assigned successful IENs to specific rural communities based on their experiences and skills. They were provided with an orientation to the organization, the local practice site, and to rural nursing practice. They were also paired with an experienced registered nurse guide/mentor for a minimum of three months. Seventy IENs from 15 different countries were recruited to work in 30 AHS hospitals, community, and long-term care sites across northern and central rural Alberta.[6]
While there is a growing body of literature on IEHPs regarding migration trends and reasons why they migrate[7, 8, 9] as well as their integration into the workforce,[10] there continues to be significant gaps in the research that examines the experiences of nurses, specifically IENs practicing in rural and remote areas.[4] The rural literature frequently explores physician experiences or combines multi-disciplinary healthcare professionals’ experiences of rural practice.[11] At times, while authors report IENs’ experiences, the context is not clearly identified or described as being rural.[12] Lastly, the term “regulated nurses’” is not clearly defined and may include experiences of registered nurses, licensed practical nurses and psychiatric nurses.[13] Hence, many questions about IENs’ experiences in rural nursing practice continue to be unanswered.
The aim of this paper is to inform practice, organizational procedures, managerial activities, and policy regarding the recruitment, integration, and retention of the rural IEN workforce in Canada.
2.Methods
A sequential mixed methods study consisted of individual interviews, photovoice approaches, and a cross-sectional survey. Multiple academic disciplines have utilized a photovoice approach to combine photographs and corresponding words/narratives produced by participants.[14] Before participating in the photovoice approach, participants completed an individual training session with one of the researchers and received digital instructional materials summarizing key training components. Study participants were asked to take photographs on their mobile cellular device of events, people, and objects that represented their experiences of rural nursing and rural life. The photographs and other related questions were discussed during the individual qualitative interview. Findings from the qualitative portion of the study are presented in this paper. The study was approved by the University of Alberta Research Ethics Office (Pro00137602) and received operational approval from AHS for a specific set of rural sites. Written consent, via DocuSign, was obtained from each IEN who participated in the individual interviews. To protect participant privacy and their anonymity and to remain compliant with ethics protocol and requirements, before the interview started, participants were asked to select a pseudonym. Participant quotes are followed by the participant’s pseudonym. To further protect participant privacy and anonymity of their responses, their characteristics are reported at an aggregate level.
2.1Sample
Newly recruited international nurses, screened and assessed by CRNA to ensure they had the skills and experience to work as a registered nurse in Alberta, arrived in groups over several months in 2023-24. As our study received AHS operational approval for only specific rural healthcare facilities in northern and central Alberta, the eligible pool of potential participants in those rural facilities was 23 IENs. Those IENs received the recruitment email via the Chief Nursing Office. Three participants initially agreed to participate in the interview, but withdrew from the study stating they had concerns with taking photographs. Two other IENs expressed interest in participating in the interview, but they did not respond to invitations for the individualized training session. Seven IENs, approximately 30.4% of the eligible pool, agreed to participate in the photovoice and related interview component. Table 1 presents the sampling details.
| Sampling Frame | *Newly recruited IENs who possess the required knowledge, competencies and experience to work as a registered nurse in a rural healthcare facility in Alberta |
| Sampling Strategy | *Purposeful sampling (Participants who possessed the characteristics described in the sampling frame and met the inclusion criteria received an invitation to participate in the study. As part of the design of the study, we needed to recruit IENs who had similar work environments and duration in their rural nursing practice, and who had participated in similar recruitment and orientation procedures.) |
| Inclusion Criteria | *Newly recruited IENs participating in AHS’ International Nurse Recruitment Initiative, started in 2023, working in a rural nursing practice at one of the operational approved sites. |
| Exclusion Criteria | *IENs working in rural nursing practice at sites not approved by AHS. *IENs hired by AHS before 2023. *IENs not employed by AHS *IENs working in urban nursing practice. |
| Recruitment Procedures | *All recruitment procedures for the study were required to follow AHS’ approval processes. *Study’s sample of IENs generated by AHS. *Chief Nursing Office of AHS distributed recruitment and reminder emails to potential IEN participants between September 2023 to September 2024 as required by the approved protocol. |
2.2Data generation
Two experienced researchers conducted semi-structured, individual in-depth interviews. When available, a graduate student took notes during the interview. Each interview lasted approximately 60 minutes and was recorded using the Zoom platform. Interview processes are presented in Table 2. Table 3 presents the interview guide.
| 1. Participant Consent Form | 1. Review the participant consent form with interviewee 2. Distribute DocuSign form for signatures 3. Outline goals of the study |
| 2. Participant Consent to Record Interview | 4. Explain method and purpose of recording 5. Obtain participant’s consent to record the interview |
| 3. Participant Pseudonym | 6. Explain reason for pseudonym 7. Record participant’s pseudonym |
| 4. Interview | 8. Start recording 9. Ask interview questions and probing questions |
| 5. Demographic Questions | 10. Ask demographic questions |
| 6. Conclusion and thank you | 11. Stop recording 12. Thank participant for participating in interview 13. Download Zoom recording to a secure environment |
| 7. Transcribe Interview Recording | 14. Digital interview recording transcribed by professional transcriptionist |
| 8. Transcription Review | 15. Transcription reviewed by two graduate students to ensure accuracy |
| Questions Regarding Transition to Living in Rural Community |
| Describe for me what your experience moving to a small rural community has been like for you. |
| Describe for me what your family’s (spouse, children, parents) experience moving to a small rural community has been like for them. |
| •How were they impacted? |
| •How were they impacted by your employment? |
| •Has your relationship with your family changed since the move and if so, how? |
| •Have their expectations been met? How so? |
| •Have your expectations been met? How so? |
| Questions Regarding Nursing Practice |
| Describe for me what your experience working in a rural hospital has been like. |
| •Describe for me what has been the most challenging aspect of your scope of practice. |
| •Describe for me what has been the least challenging aspect of your nursing practice. |
| Questions Regarding Transition to Rural Nursing Practice |
| •What steps/actions/behaviours did you take to enhance your resilience (ability to cope/adjust/adapt) while working in a rural nursing practice? |
| Questions Regarding Integration into the Rural Community |
| •What steps/actions/behaviours did you take to facilitate your integration and acceptance into the community? |
| Questions Regarding How Their Experience Could be Enhanced |
| •What recommendations would you make to enhance/improve your experience of moving to Alberta to work as a rural nurse? |
2.3Data analysis
The researchers independently conducted inductive thematic analysis of the qualitative data, following a multi-step approach to identify patterns and themes (see Table 4).
| Independent Analysis | Two researchers independently followed the analysis process: 1. Read and reread transcripts for overall understanding 2. Generate initial codes 3. Group similar codes into categories and subcategories 4. Refine categories and subcategories 5. Identify and define tentative themes supported by categories and subcategories 6. Analyze themes in relation to study’s research questions 7. Repeat each above step after team review and discussion (3 rounds total) |
| Team Review and Discussion (3 cycles) | Two researchers jointly: 8. Review and discuss their independent findings 9. Reach consensus on emergent themes, categories and subcategories 11. Agree on themes, categories and subcategories: extremely high level of agreement between two researchers 10. Repeat steps 8 and 9 |
| Last Procedure | *Map themes and their definitions, and categories and subcategories with relevant quotes to summary table |
3.Results
Table 5 presents participant demographic data. Participants in this study immigrated from several countries. All the participants were married and indicated that their spouse and children had immigrated with them. While there was a range of years of nursing practice experience among the participants, the years of experience did not seem to influence the types of challenges they encountered or how they navigated these challenges. Lastly, all the participants were relatively new to rural Alberta having started their employment within nine months of participating in this study. The qualitative findings presented below may reflect the ‘newness’ of their transition and integration.
| Size of Sample | *n = 7 IENs participated in the photovoice with individual interviews |
| Sample Characteristics | *Migrated to Canada from: Asia, Africa, and North America *Age range: 25 to 44 years of age *Marital status: all participants were married *Gender: 3 females and 4 males *Nursing education: Baccalaureate degree in nursing or graduate education; completed in English *Years of experience prior to Alberta position: 6 to 20 years *Prior rural nursing experience prior to Alberta position: 2 participants *Length of time in Alberta position: 3 to 9 months |
Qualitative data analysis of the interview transcripts, photographs, and photographic statements resulted in two broad themes (see Table 6). Thriving in Rural Nursing Practice presents the participants’ experiences of adjusting to rural nursing practice. They discuss the challenges they encountered and the strategies they used to overcome these challenges. The second theme, Rurality, describes the challenges they encountered relocating to the rural community. This section concludes with strategies the participants used to help them integrate into their new rural environment. Each theme is supported by categories and direct participant quotes.
| Analysis Results |
*Two themes with multiple categories and subcategories: |
3.1Thriving in rural nursing practice
Throughout the theme of thriving in rural nursing practice, the categories point to what rural nursing practice is like for the participants. There are two broad categories: wider scope of practice and becoming part of a team. Each category is supported by sub-categories and direct participant quotes.
3.1.1Wider scope of practice
Consistent with the literature, study participants talked about how their scope of practice changed to meet the health care needs of community members.[15, 16] For the participants, like expert generalists, this meant working in “in all spaces” (Possible) that is, in multiple patient care areas with patients across the lifespan, who have a myriad of health challenges.[17, 18, 19] They also quickly realized that there were limited resources (human and material) which meant they identified “lifelines” (Jason) like telephones, text messaging, and access to paramedics to provide safe patient care. However, because they might not have worked in some patient care areas or their experience was a bit dated, to adjust to a wider scope of practice, the participants explained having to assess their own knowledge and skill level to provide safe patient care.
To meet the challenge of having a wider scope of practice with limited resources, the participants discussed some strategies they independently used to refresh their competencies like engaging in independent reading, observing how colleagues completed various tasks, and asking questions. They were also very willing and happy to engage in learning opportunities their employer provided to advance their knowledge and competence.
One participant stated it was essential and helped to bolster her confidence when their work buddies were immigrants who understood the challenges of integrating into the work environment and anticipated her needs.
Although all the participants recognized the importance of maintaining and/or advancing their level of competency because of the generalist practice required in rural hospitals, they also point out that they come to their role with pre-existing skills and knowledge. Because of that, they can and are, contributing team members.
Sometimes though, even if the participant possesses knowledge and skills that can contribute to patient care, the workplace environment does not recognize their competence.
For some participants where their level of competence was always being evaluated and questioned and where there was limited support from colleagues, the potential to doubt themselves resulted in putting their mental health at risk.
3.1.2Becoming part of the team
Adjusting to cultural norms that were different from their previous experience of being part of a healthcare team was expected although there were some “professional surprises…when you see people who believe things differently from the way you believe and see things” (Wendy). Against this background, the participants also recognized the importance of establishing good working relationships with their colleagues since becoming part of the team was not a given: it was a process that required support from managers, colleagues, and particularly their registered nurse guide/mentor. Indeed, their guide/mentor seemed to have a significant influence on participants’ ability to become part of the team by assisting them to navigate expectations of the nurse’s role.
Along with having a preceptor/mentor, the participants spoke about the importance of connecting with other IENs working in the facility. They explained that these more experienced IENs understood the challenges they were facing and could provide guidance on navigating them.
The participants were also acutely aware that to become part of the team they needed to take initiative in establishing relationships with their colleagues albeit at times, they used caution: I know that I should open up to the extent that I know [it]will not come back to backfire on me (Possible). Consequently, they were able to clearly identify instances that for them, demonstrated they had become a member of the team.
Unfortunately, though, the consequences of not being able to become a member of the team could be devastating for the individual and a loss for the hospital and community.
3.2Rurality
The second theme that was generated is rurality. The concept of rural often includes a combination of geography, culture, population size or density, and qualitative experience.[20] It can also be described as a state of being rooted in relationship because “people, ideas, and goods flow between urban and rural settings, connecting people and places in diverse ways and across a range of scales”(p. 268).[21] For the participants in this study, the experience of being rural included practical aspects like adjusting to the cold weather and dealing with scarce housing to more psychosocial aspects like adjusting to a new environment and community. This theme is supported by two categories: challenges of relocating to a rural community and integrating into the community.
3.2.1Challenges of relocating to a rural community
Relocation challenges varied among the participants, which might reflect the geographical location of the rural community, its size, and available amenities like public transportation (Peter) or not having a Costco (Brad). That said, the most challenging aspect of relocating to small rural communities every participant spoke about, was the scarcity of appropriate housing. The scarcity of housing resulted in one participant having to border with a local family for a time in “order to survive” (Lisa). The scarcity of housing also created financial burdens as well as extensive stress for the participants and their families. If participants were more tentative about permanently moving to the rural community, they quickly found out that finding a rental was very difficult as well as financially stressful especially if they also retained some form of accommodation in the city.
Along with limited housing options, the participants shared challenges related to finding employment opportunities for their spouse either because of language barriers or because employment was only feasible in large cities. These challenges resulted in families living apart from one another.
Two participants with young children found the limited number of childcare programs or the time of year they relocated, meant childcare was difficult to secure.
Although the harshness of winter is not unique to rural Alberta, all the participants spoke of needing to adjust to a Canadian winter. While they appreciated the beauty of what a winter day can bring, they also spoke of the dangers and possible isolation because of the winter conditions.
The last challenge the participants spoke about regarding relocating to rural Alberta, dealt with being an ‘outsider’. As visible minorities, entering predominantly Caucasian Christian communities required patience and fortitude from all family members. For one participant, if at some point in their journey they felt that the community could not accept them, they would leave.
3.2.2Integrating into the community
The participants in this study were committed to making their move to rural Alberta successful. For at least one participant, the connections they made with professional colleagues was a conduit to creating relationships within the community. Others participated in community events to connect to the community.
The participants were also quick to point out that two other factors helped facilitate their transition and integration into the community. The first was the support their employer provided them by linking them to key community members who had social capital as well as providing practical guidance for becoming part of the community.
The second factor that helped them transition and integrate into the community was the support from family and friends who were going through similar experiences.
Although tempered by cold winter weather, the natural beauty that surrounded their local community and how that natural beauty extended into their workplace, impacted the participants’ experience of integration into the community.
Wide open spaces, sparse traffic, and fewer people created a sense of physical safety for some participants enhancing the appeal of living in rural Alberta.
4.Discussion
Results from the individual interviews highlight two main themes: (1) Thriving in Rural Nursing Practice and (2) Rurality. These themes and their related categories describe mostly positive aspects of IENs’ transition to the rural nursing setting and community although one IEN describes negative consequences because of her experiences. For this participant, mental health risks and leaving rural nursing practice and the rural community ensued when their competencies were not recognized. Hence, the participant was unable to become a member of the healthcare team.
The Thriving in Rural Practice theme includes two categories – Wider scope of practice and Becoming part of a team. The category of Wider scope of practice describes what rural nursing practice is like for the IENs and their actions and strategies which echoes much of the extant literature regarding having a broad generalist and demanding scope of practice.[22, 23, 24] To adjust to the wider scope of practice and to meet the healthcare needs of their patients “in all spaces,” the participants drew upon their own knowledge and skill and learned how to navigate the differences between their home country’s healthcare practices and rural nursing practice in Canada. Along with engaging in self-learning, IENs viewed access to professional development and learning opportunities (e.g., organization study guides, procedural manuals), and mentoring[24] as essential for them to be successful in their new employment. According to Mbema et al,[25] information and communications technologies like telehealth have positive impacts on recruitment and retention of nurses to rural practice by reducing professional isolation. Participants in this study describe lifelines (for example telephones) as support mechanisms for the provision of safe patient care. Although professional isolation appears in the extant literature, according to Williams,[26] the concept is poorly described or defined and limited to geographic or social aspects. More recently, Hunt and Hunt[27] described it as the lack of frequent and effective communication between healthcare providers. It would be important therefore, that as part of their onboarding, IENs be provided a structured and comprehensive orientation[28] to the workplace including various information and communication technologies like Connect Care, platforms for secure text messaging, and instructions on how to contact their supervisors, especially when off-duty or off-site.
Consistent with the findings from Alexis, Vydelingum, and Robbins[28] and Omeri and Atikins,[29] participants in this study indicated that their knowledge and skill and at times practice experience were either undervalued or simply not valued at all by managers and other nurses. To enhance IENs’ self-esteem and engender confidence in their ability to provide safe patient care in such complex practice settings like rural hospitals, managers, nurse educators, and organizational leaders should take on more proactive responsibility for encouraging the acquisition of nursing competencies. For example, pre-screening IENs knowledge and skill at pre-hire, assessing and reassessing knowledge during orientation, and targeting in-service training to address unique and specific knowledge and skill deficits are some strategies that can help IENs develop a wider scope of practice and may help retain this workforce.[30] Clinical nurse educators should also be encouraged to take a preceptorship course like that offered by the Canadian Association of Schools of Nursing as well as other pedagogical courses focusing on how to teach, mentor, and preceptor healthcare professionals using a culturally sensitive and trauma-based approach.
Another unique finding is the connection IENs sought with colleagues, who are also immigrants (described as “work buddies”) because of their reassurance and abilities to relate to their professional challenges and situations. Seeking someone out who has similar experiences may have been in response to what Omeri and Atkins[29] describe as “othering” (p.503) where social and cultural distancing occurs between nurses of the dominant culture and immigrant nurses from culturally and linguistically diverse backgrounds. To help IENs transition to rural nursing practice and to assist receiving facilities in acclimating to a more diverse workforce, it may be helpful for managers to encourage and lead self-reflection sessions with staff members. These sessions could explore attitudes, beliefs, and assumptions about IENs and the effects these personal views have on interactions with colleagues, patients, caregiving, and healthcare delivery. Employers could also deliberately place newly hired IENs in settings where there are other IENs. This would perhaps create a natural transition bridge for the newly hired IENs.
As part of Becoming Part of the Team, in small rural and remote communities where healthcare teams may be small, team dynamics, everyday practice experiences, and available workplace supports can influence IENs commitment to the organization[31] and overall job satisfaction.[32] In this study, IENs note that the concept of becoming part of the team is not automatic and/or assured; instead, it requires supportive relationships through mentoring, clinical supervision, and preceptoptoring.[25] Becoming part of the team is also a shared responsibility that IENs need to initiate and that their team members need to acknowledge through a specific action or recognition activity (e.g., in one instance, a participant’s name was written on a Christmas stocking displayed in the hospital along with other team members Christmas stockings). To deconstruct the monoculture[29] that exists, and to cultivate a culture of friendliness and acceptance,[29] receiving facilities and communities as well as IENs need to learn about communication norms, engage in deliberate activities that support exploration of cultural practices as well as social activities. Based on the findings of this study, it is apparent the fit of the nurse with the realities of rural practice is important for retention[31] since the negative consequences of not becoming part of the team might result in IENs making the decision to leave the rural hospital and community.
The study’s theme of Rurality enriches the concept of “rural” as described above by Chalmers and Joseph[20] and Herron and Skinner.[21] In this study, rurality encompasses two categories – Challenges of relocating to a rural community and Integration into community. The IENs describe various challenges from practical aspects such as scarce housing and limited shopping options to adjusting to extreme cold temperatures, limited childcare options, and limited or non-existent employment for their spouses. Resource limitations plus the dangers and isolation of winter conditions compared to IENs’ expressions of the natural beauty of the surroundings of their local communities, the diverse wildlife, and one’s sense of physical safety create a juxtaposition and important finding. Indeed, it speaks to the need of recruitment officers, nurse leaders, and community members to provide more detailed information regarding housing, employment opportunities, school schedules, and childcare options to IENs considering immigrating to Canada and in particular rural Alberta. Recruitment officials might also engage in more strategic recruitment regarding the timing of IENs’ relocation so that the transition is a bit easier for them and their families.
The category of Integrating into the Community highlights the commitment of IENs to adjust to rural settings in Alberta. Affective commitment (commitment associated with a sense of belonging and emotional attachment) is particularly important in rural settings where professional and personal lives intersect and intertwine, and where the healthcare facility is often a major component of the community.[31] Thus, relationships with professional colleagues, connecting to community members with social capital, and participation in community events may help to create relationships with community members.[23]
Strengths and limitations
The strengths of this study include its rich, deep, and nuanced qualitative data set, findings that are consistent with results in the published literature, and other findings that provide new insights about IENs’ experiences, strategies and actions when transitioning and integrating into rural nursing settings. Another important strength of this study is it starts to address significant gaps in the research exploring and investigating the experiences of IENs practicing in rural and remote areas in Canada. The findings from this study most likely will generalize to other rural and remote areas within and outside of Canada. Finally, some of the results from this study add to and expands upon the body of literature regarding nursing practice in rural and remote areas.
This study also has limitations that need to be considered: 1) The sample was limited to seven IENs’ experiences working in a sub-set of rural care facilities in Alberta, Canada; 2) Recruitment of participants was allowed in only 15 AHS rural sites through their Chief Nursing Office; and 3) All rural sites were in central and/or northern Alberta which might impact the applicability of the findings to other rural and/or geographical locations. It is possible that rural experiences in southern Alberta are different because there is a higher population density and proximity to urban centers. Although there were two participants who had rural experience in their home countries, it is possible that their previous experience influenced their experience of rural nursing practice in Alberta. Moreover, the sample was limited to registered nurses (RNs). Future research would benefit from the inclusion of multiple perspectives (such as nurse colleagues, mentors, and managers) and multiple levels (such as unit, facility, and organization) to develop a more comprehensive understanding of IENs’ experiences (see Figure 1).
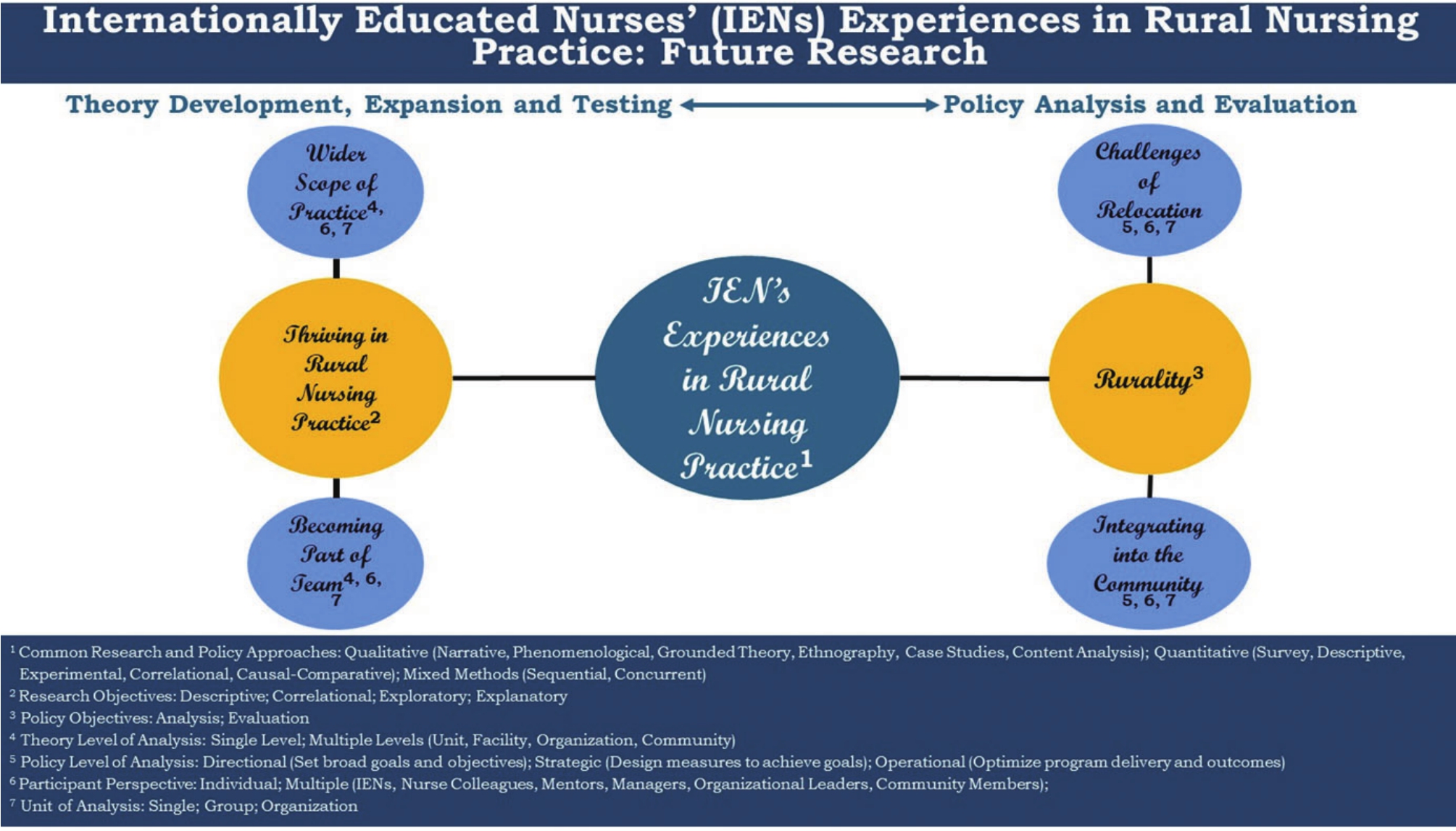
Figure 1.
Future research
Lastly, due to the physical distance between rural locations and the time constraints of participants, we used the platform, Zoom, to conduct virtual interviews. Although virtual interviews might result in the inability to establish rapport with the participants and problems with internet connectivity, the study’s semi-structured interview protocol provided a mechanism to establish rapport with each participant and set the stage for a rich two-way conversation in the virtual environment. We did not experience any internet connectivity issues while conducting the interviews. IENs expressed they used a variety of digital tools to connect with distant family members and to complete continuing education opportunities, which demonstrated their comfort level, familiarity, and use of ubiquitous virtual platforms.
5.Conclusion
IENs are a valuable resource for the sustainability of the Canadian nursing workforce particularly in rural settings. While this study presents findings that are consistent with the rural nursing literature as well as the literature on IENs, this study also contributes valuable insights into potential actions, activities and strategies for recruiting, integrating and retaining IENs in rural nursing practice. Organizations and their recruitment teams need to develop a strategic approach when recruiting IENs. Careful attention needs to be given to addressing practical issues like availability of housing, employment opportunities for family members, childcare options and school schedules, and detailed information regarding amenities. Policies and procedures that address the monocultural ethos in the workplace and community need to be developed, implemented, assessed for their effectiveness in creating a friendly and accepting environment. Mentoring opportunities and connecting recent IEN immigrants to IEN who have been in the country and working in the workplace would help with IENs’ adjustment and transition. Lastly, a comprehensive program for the development of rural nursing practice competencies that recognizes IENs pre-existing skills and knowledge needs to be implemented at the organizational and practice site levels.
Authors contributions
Dr. Sedgwick and Dr. Kelley contributed equally to the study and were responsible for study design and revising, and data collection. Both Dr. Sedgwick and Kelley drafted, revised, and approved the final manuscript.
Funding
This work was funded by Rural Health Professions Action Plan (RhPAP).
Conflicts of Interest Disclosure
The authors declare they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Informed consent
Obtained.
Ethics approval
This study was approved by the University of Alberta Research Ethics Office (Pro00137602). The Publication Ethics Committee of the Association for Health Sciences and Education. The journal’s policies adhere to the Core Practices established by the Committee on Publication Ethics (COPE).
Provenance and peer review
Not commissioned; externally double-blind peer reviewed.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Data sharing statement
No additional data are available.
Acknowledgements
Not applicable.
References
- Canadian Institute for Health Information (CIHI). The state of the health workforce in Canada, 2023 [Internet]. 2025 June 26. https://www.cihi.ca/en/the-state-of-the-health-workforce-in-canada-2023/health-workforce-recruitment-and-retention
- Covell C, Adhikari A, Salami B. Surviving the employment gap: a cross-sectional survey of internationally educated nurses. Int. Nurs. Rev. 2022;69(2):167-174. PMID:33687068 doi:10.1111/inr.12668
- Lee R, Wojtiuk R. Transition of internationally educated nurses into practice: what we need to do to evolve as an inclusive profession over the next decade. Nurs. Leadersh. 2021;34(4):57-64. PMID:35039119 doi:10.12927/cjnl.2021.26689
- Dywili S, Bonner A, Anderson J. Experience of overseas-trained health professionals in rural and remote areas of destination countries: a literature review. Aust. J. Rural Health. 2012;20(4):175-184. PMID:22827424 doi:10.1111/j.1440-1584.2012.01281.x
- College of Registered Nurses of Alberta (CRNA). Current registration in one of these jurisdictions [Internet]. 2025 June 26. https://connect.nurses.ab.ca/home/
- Alberta Health Services. Newly recruited international nurses arriving in province [Internet]. 2025 June 26. https://www.albertahealthservices.ca/news/Page17723.aspx
- Buchan J, Sochalski J. The migration of nurses: trends and policies. Bull World Health Organ. 2004;82(8):587-594. PMID:15375448
- Kingma M. Nurses on the move: historical perspective and current issues. OJIN. 2008;13(2). Man 01 doi:10.3912/OJIN.Vol13No02Man01
- MacKay S, Smith A, Kyle R. What influences nurses’ decisions to work in rural and remote settings? A systematic review and meta-synthesis of qualitative research. RRH. 2021;21:6335. PMID:33653078 doi:10.22605/RRH6335
- Alostaz N, Walton-Roberts M, Chen R. Integration trends of internationally educated nurses in Canada and Australia: a scoping review. IHTP. 2024;4(1):88-113. doi:10.32920/ihtp.v4i1.1958
- Safari K, McKenna L, Davis J. Transition experiences of internationally qualified health care professionals: a narrative scoping review. Int. J. Nurs. Stud. 2022;129:104221. PMID:35349971 doi:10.1016/j.ijnurstu.2022.104221
- Higginbottom G. The transitioning experiences of internationally educated nurses into a Canadian health care system: a focused ethnography. BMC Nursing. 2011;10:14. PMID:21693059 doi:10.1186/1472-6955-10-14
- Covelle C, Adhikari A, Salami B. Surviving the employment gap: a cross-sectional survey of internationally educated nurses. Int. Nurs. Rev. 2022;69(2):167-174. PMID:33687068 doi:10.1111/inr.12668
- Breny J, McMorrow M. Photovoice: an introduction to the method and analysis tips [Internet]. Sage Research Methods Community. 2025 June 26. https://researchmethodscommunity.sagepub.com/blog/photovoice-an-introduction-to-the-method-and-analysis-tips
- Lankshear S, Martin D. Getting comfortable with “It depends”: embracing the impermanence of scope of practice. Nurs. Leadersh. 2019;32(1):30-41. PMID:31228343 doi:10.12927/cjnl.2019.25850
- MacLeod M, Stewart N, Kosteniuk J. Rural and remote registered nurses’ perceptions of working beyond their legislated scope of practice. Can. J. Nurs. Leadersh. 2019;32(1):21-31. PMID:31228342 doi:10.12927/cjnl.2019.25851
- MacLeod M, Martin-Misener R, Banks K. ‘I’m a different kind of nurse’: advice from nurses in rural and remote canada. Can. J. Nurs. Leadersh. 2008;21(3):40-53. PMID:18815470 doi:10.12927/cjnl.2008.20060
- Ayers R. Rural nursing, concepts, theory, and practice. Edited by Winters C, Lee H. New York, NY; Springer Publications New York. 2010: 269-284.
- Muirhead S, Birks M. Roles of rural and remote registered nurses in Australia: an integrative review. Aust. J. Adv. Nurs. 2019;37(1):21-33. doi:10.37464/2020.371.5
- Chalmers A, Joseph A. Handbook of rural studies. Edited by Cloke P, Marsden T, Mooney, P. Thousand Oaks, CA; Sage Publications Ltd. 2006: 388-400. doi:10.4135/9781848608016.n28
- Herron R, Skinner M. Routledge handbook of health geography. Edited by Crooks V, Andrew G, Pearce J. London, England; Routledge. 2018. doi:10.4324/9781315104584
- Molinari D, Monserud M. Rural nurse job satisfaction. Rural Remote Health. 2008;8(4):1055. PMID:19061306 doi:10.22605/RRH1055
- Sutton K, Waller S, Fisher K. Understanding the decision to relocate rural amongst urban nursing and allied health students and recent graduates. 2016.
- Holland C, Malatzky C, Pardosi J. What do nurses practising in rural, remote and isolated locations consider important for attraction and retention? a scoping review. Rural Remote Health. 2024;24:8696. PMID:39307544 doi:10.22605/RRH8696
- Mbemba G, Gagnon M, Pare G. Interventions for supporting nurse retention in rural and remote areas: an umbrella review. HHR. 2013;11(44). PMID:24025429 doi:10.1186/1478-4491-11-44
- Williams M. Professional isolation: an integrative review. J. Rural Nurs. Health Care. 2012;12(2):3-10. doi:10.14574/ojrnhc.v12i2.51
- Hunt S, Hunt E. Barriers to practice of rural and remote nursing in Canada. ESJ. 2016;12(36):56. doi:10.19044/esj.2016.v12n36p56
- Alexis O, Vydelingum V, Robbins I. Engaging with a new reality: experiences of overseas minority ethnic nurses in the NHS. J. Clin. Nurs. 2007;16(12):2221-2228. PMID:18036112 doi:10.1111/j.1365-2702.2007.02080.x
- Omeri A, Atkins K. Lived experiences of immigrant nurses in New South Wales, Australia: searching for meaning. Int. J. Nurs. Stud. 2002;39(5):495-505. PMID:11996870 doi:10.1016/S0020-7489(01)00054-2
- Aqtash S, Robb W, Humter L. Self-assessed competence of experienced nurses in a rural and remote setting. Nurs. Open. 2017;3:1-17. doi:10.1177/2377960817702382
- Stewart N, D’Arcy C, Kosteniuk J. Moving on? Predictors of intent to leave among rural and remote RNs in Canada. J Rural Health. 2011;27(1):103-13. PMID:21204977 doi:10.1111/j.1748-0361.2010.00308.x
- Hegney D, McCartby A, Rogers-Clark C. Retaining rural and remote area nurses. The Queensland, Australia experience. JONA. 2002;32(2):128-135. PMID:11984243 doi:10.1097/00005110-200203000-00005
 This work is licensed under a
This work is licensed under a 