1.Introduction
Burnout is on the rise among healthcare providers. Since the onset of the COVID-19 pandemic, Certified Registered Nurse Anesthetists (CRNAs) and Student Registered Nurse Anesthetists (SRNAs) have been particularly susceptible due to the role’s inherent stress. In a study conducted at a level one trauma center, researchers identified that 72% of CRNAs experienced some degree of burnout.[1] Burnout is defined as a complex human experience characterized by emotional exhaustion, loss of personal fulfillment, and depersonalization.[2] Emotional exhaustion is characterized by feeling depleted of emotional resources. Loss of personal fulfillment is a decreased sense of accomplishment either professionally or personally. Depersonalization in healthcare is a term used to describe cynicism or lack of empathy towards patients or colleagues.
This phenomenon has deleterious effects on providers, healthcare organizations, and patient safety. Balayssac et al. examined 1,322 French healthcare providers and identified that burnout was associated with significant mental health comorbidities such as anxiety, depression, and substance abuse.[3] Mahoney et al. found CRNAs who suffer from burnout are more likely to quit their jobs, a trend which leads to increased staff turnover which can result in enormous costs to organizations.[4] After examining direct and indirect costs of turnover, authors estimated the average figure to replace an experienced CRNA to be $145,000 to $157,000.
Burnout also poses a threat to patient safety. One study examined 1,508 physician anesthesiology residents throughout the United States and studied the effects of burnout on adherence to best practice guidelines.[5] Physician anesthesiology residents who experienced elevated levels of burnout had increased deviation from best practices of care compared to those residents with low levels of burnout (
The first purpose of this project was to examine and compare burnout scores among CRNAs and SRNAs working at a large, academic, level one trauma center via the Maslach Burnout Inventory – Human Services Survey for Medical Personnel (MBI-HSS) to further define the needs of this population. The second purpose of this project was to compare burnout between the three SRNA cohorts within a nurse anesthesia program. This project used results of the MBI-HSS to develop a discussion disseminated via a two-part podcast series.
2.Methods
To address ethical considerations with implementation, data collection, data analysis, and dissemination, this project was reviewed by the University Institutional Review Board and received approval for the non-human subjects research protocol. There are no conflicts of interest to disclose. Rights to usage and licenses to administer the MBI-HSS were purchased through Mind Garden, Inc., an international publisher of psychological assessments and an industry leader in providing tools to facilitate positive organizational transformation. Funding to purchase the tool’s license agreement was acquired through a university grant awarded to the examiners.
Investigators created a wellness assessment which incorporated the MBI-HSS tool and gathered participant demographic data. The MBI-HSS, developed by Christina Maslach in 1981, is a twenty-two-item questionnaire that has been used extensively to evaluate burnout among healthcare workers, students, educators, and human services workers.[6] It is considered the gold standard for assessing burnout and has demonstrated high reliability with a Cronbach alpha score of > 0.70.[7] Examples of MBI-HSS questions are listed in Table 1. MBI-HSS creators prohibit publishing the entire instrument to maintain its integrity.[8]
| Emotional Exhaustion (EE) | I feel emotionally drained from my work. |
| Personal Accomplishment (PA) | I have accomplished many worthwhile things in this job. |
| Depersonalization (DP) | I do not really care what happens to some patients. |
The MBI-HSS was initially developed as a burnout assessment tool that examined the three subscales of burnout: emotional exhaustion (EE), depersonalization (DP), and personal accomplishment (PA) and categorized subscale scores into three groups: low, moderate, and high (see Table 2).[6] For the EE subscale, scores were categorized as low burnout (< 17), moderate burnout (18-29), and high burnout (> 30). DP scores were categorized as low (< 5), moderate (6-11), and high burnout (> 12). High PA scores are considered protective of burnout: scores (> 40) indicate low burnout, scores of 34-39 indicate moderate burnout, and scores < 33 indicate high burnout .[9]
| Low degree | Moderate Degree | High Degree | |
| Low degree | Moderate degree | High degree | |
| Low degree | Moderate Degree | High degree |
Investigators created an assessment, titled “Wellness Survey”, to administer the MBI-HSS questionnaire. Maslach and Jackson recommend using the title “Wellness Survey” and to avoid using ‘burnout’ in an MBI-HSS assessment title which may increase sensitization to the term.[8] In addition to the MBI-HSS, the Wellness Survey also asked participants to self-report if they belonged to the CRNA or SRNA group. For the CRNA group, participants were asked to report their years of work experience as a CRNA, how many hours they are scheduled to work each week, and how many hours of overtime they worked in the last month via a Likert scale. For SRNAs, participants were asked to select which cohort within the nurse anesthesia program they belonged to: SRNA1, SRNA2, or SRNA3. At the survey’s end, participants were asked via a free text response to share any strategies or activities they use to manage stress.
The license agreement from Mind Garden, Inc. explicitly states that the MBI-HSS may only be used for research purposes and individual burnout scores are not to be shared with participants as this may affect the integrity of the survey.[8] However, the inability of survey takers to see their burnout scores is a limitation of this project as this data would be insightful for CRNAs and SRNAs.
The Wellness Survey was implemented at a large urban, academic, level 1 trauma center with 724 licensed patient care beds. The academic medical center has 34 main ORs and other anesthetizing locations including interventional radiology, catheterization lab, endoscopy, cystoscopy, electrophysiology, and obstetrics. The population chosen consisted of CRNAs of various years of experience who worked PRN, part-time, or full-time and SRNAs in their first, second, and third years of education. Physician anesthesiology attendings, physician anesthesiology residents, and certified anesthesia assistants were not included in the population surveyed.
To disseminate the MBI-HSS to respondents, the survey was imported into RedCap Survey Services, a scientific data management and survey tool. To ensure confidentiality, an administrator not affiliated with the project sent an email to all CRNAs and SRNAs with a link to the survey. The CRNAs were provided with a QR code which, when scanned with a mobile device, directed them to the Wellness Survey. Data from the survey was exported to Microsoft Excel where statistical analysis was conducted. Descriptive statistics were used to summarize the CRNAs’ demographic data and describe SRNA cohort representation. Measures of central tendency were calculated for each of the three sections of the MBI-HSS for both CRNAs and the collective SRNA group. A t-test was performed to compare MBI-HSS results between CRNAs and SRNAs using a 95% confidence interval. Measures of central tendency were calculated for each SRNA cohort’s MBI-HSS scores to further explore differences in burnout among the three cohorts.
After statistically analyzing the data of the Wellness Survey, a two-part podcast was recorded and edited with the assistance of the university broadcast and podcast innovation hub. The two-part series was published to two major podcast services – Apple Podcasts and Spotify Podcasts – for easy public access (see Figure 1). Dissemination of Wellness Survey results were discussed by investigators in each episode. The first episode defined burnout and its implications for practice. Mitigation strategies to combat burnout which were collected in the free narrative of the survey were discussed along with the CRNA data results. This episode also includes an interview with a currently practicing CRNA of 8 years who gives personal testimony on how burnout has impacted her career. The second episode delves into the SRNA data. An interview with a practicing CRNA of four years explores the stress of attending a nurse anesthesia program and the transition from SRNA to CRNA. Evidence-based strategies to combat burnout, such as mindfulness activities, and campus resources were also presented.
Figure 1.
QR codes for Apple podcasts and spotify
3.Results
Ninety-one respondents completed the Wellness Survey. Thirty-two respondents were CRNAs (see Table 3) with the remaining 59 survey-takers being SRNAs (see Table 4). When examining the average number of clinical hours scheduled per week among CRNAs, 96.9% reported working over 30 hours per week. When examining those CRNAs working overtime (over 40 hours) during a month, 50% worked 13 or more hours per month. The survey also asked CRNAs to report their years of work experience as a CRNA. Of the 32 respondents, 75% reported working as a CRNA for greater than 5 years.
| Years of CRNA work experience | ||
| < 1 | 1 | 3.1 |
| 1-3 | 7 | 21.9 |
| 4-9 | 9 | 28.1 |
| 10+ | 15 | 46.9 |
| Average hours scheduled per week | ||
| < 20 | 0 | 0 |
| 20-30 | 1 | 3.1 |
| 30-40 | 18 | 56.3 |
| > 40 | 13 | 40.6 |
| Hours of overtime worked in last month | ||
| 0 | 8 | 25 |
| 1-12 | 8 | 25 |
| 13-23 | 9 | 28.1 |
| > 24 | 7 | 21.9 |
| Year in Training | ||
| SRNA1 | 17 | 28.8 |
| SRNA2 | 23 | 39.0 |
| SRNA3 | 19 | 32.2 |
The SRNA respondents were stratified into cohort classifications (i.e. year 1, 2 or 3). A breakdown of the mean MBI-HSS scores for each SRNA cohort is displayed in Table 5. All three SRNA cohorts scored in the moderate range of burnout for emotional exhaustion (EE). SRNA3s had the highest EE score (27.21) with SRNA1s having the second highest EE score (23.35). When examining depersonalization (DP) scores, all three cohorts scored in the moderate range of burnout. SRNA1s demonstrated the highest DP score (11.12). For personal accomplishment, SRNA1s had the highest sense of personal accomplishment compared to the other two cohorts.
| Emotional Exhaustion | SRNA1 | 23.35 |
| SRNA2 | 22.91 | |
| SRNA3 | 27.21 | |
| Depersonalization | SRNA1 | 11.12 |
| SRNA2 | 5.00 | |
| SRNA3 | 8.26 | |
| Personal Accomplishment | SRNA1 | 35.47 |
| SRNA2 | 32.48 | |
| SRNA3 | 31.89 |
Figure 2 displays the mean MBI-HSS scores for CRNAs and the combined SRNA group. A
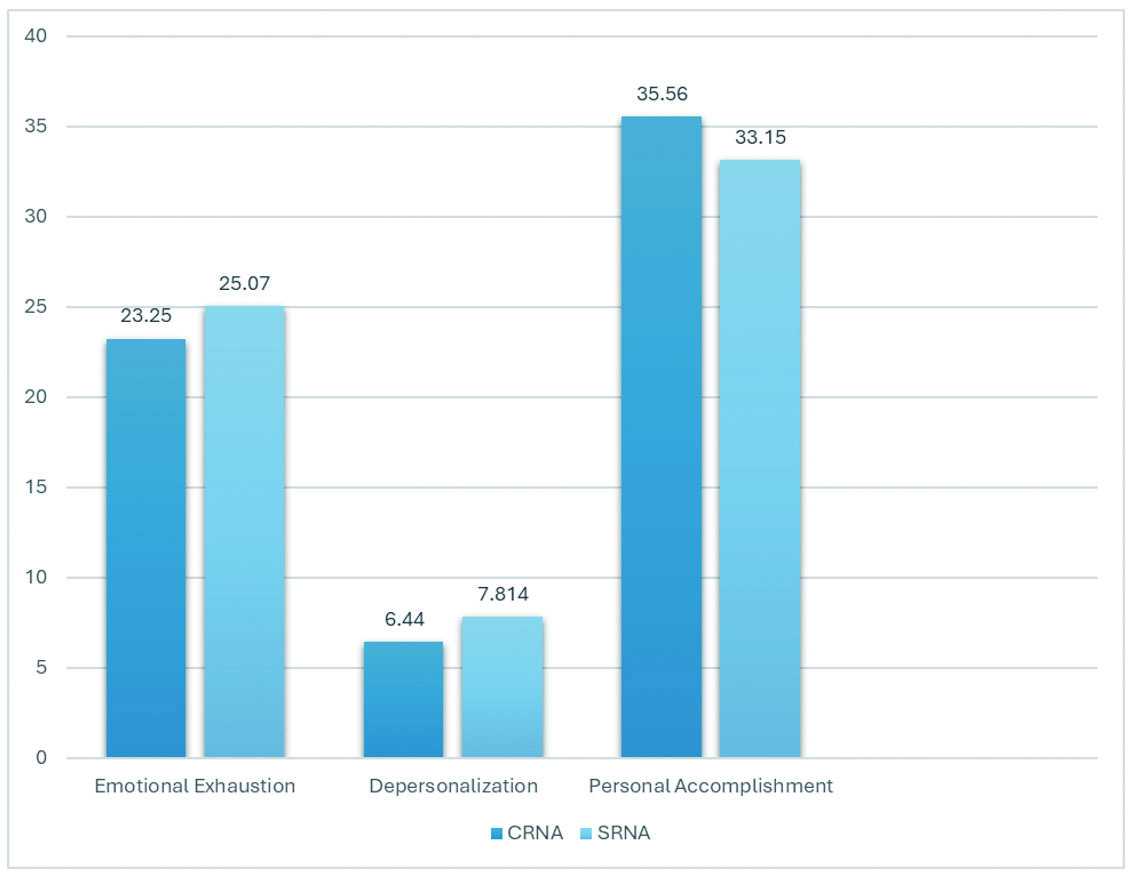
Figure 2.
Comparison of mean MBI-HSS scores between CRNAs and SRNAs
4.Discussion
The purpose of this project was to evaluate and compare burnout levels among CRNAs and SRNAs working at a large academic medical center and to increase awareness of the consequences of burnout through a two-part educational podcast. This project is among the first to explore how burnout varies between CRNAs and SRNAs and examine how burnout differs between SRNA cohorts.
Survey results indicate that both CRNA and SRNA survey-takers reported a moderate degree of burnout. This underscores the importance of developing healthy coping mechanisms during SRNA training that can be carried into one’s career as a CRNA. The demographic questionnaire for CRNA survey respondents offers additional insight. Many CRNA respondents (46.9%) reported ten or more years of work experience as a CRNA. This suggests burnout incidence may increase as one’s career develops. Additionally, 40.6% of CRNA respondents reported working over 40 hours (about 3 days) each week, with 75% of the CRNAs working some amount of overtime in the last month. This is not surprising when considering the short-staffed nature of the clinical site following the COVID-19 pandemic. This may become a significant problem if anesthesia job vacancy rates increase. Future projects may explore how working overtime affects burnout in CRNAs.
Examining the scores of the three realms of burnout sheds light on vulnerabilities within the SRNA respondents. Interestingly, SRNA1s had the highest depersonalization scores compared to SRNA2s and SRNA3s. SRNA1s completed the survey in the second month of the thirty-six-month program. One explanation for high depersonalization scores among SRNA1s is this group recently resigned from high-stress jobs working as critical care ICU nurses. In this role these individuals were considered “experts.” This is a sharp contrast to becoming a novice anesthesia provider. Their scores may also be reflective of residual burnout from their jobs at the beside. SRNA1s also attend online courses this first semester, which may be isolating, contributing to increased depersonalization. SRNA3s had the highest scores for emotional exhaustion, as they are nearing the end of a long, arduous program. As SRNA3s prepare to graduate and step into the CRNA role, they are already reporting a significant degree of burnout. Future exploration may focus on examining the experience of new graduate CRNAs as they transition from SRNA to CRNA. Additionally, exploring ways to decrease burnout between graduation and starting one’s career may be beneficial.
The SRNA groups reported a low sense of personal accomplishment compared to CRNAs, particularly in SRNA2s and SRNA3s. This is understandable as CRNAs have completed their training and have reached their goal of working as an anesthesia provider. SRNA1s had the highest personal accomplishment scores of all students. This may be related to achieving admission to a nurse anesthesia program. Surprisingly, personal accomplishment scores decreased as trainees progressed in the program. The Dunning-Kruger Effect offers one explanation for decreasing personal accomplishment scores as students progress through the program. David Dunning and Justin Krueger, two psychologists, conducted four studies to examine college students’ perceptions of their own performance.[10] They suggest that novices are much more likely to overestimate their skills and proficiency when compared to their more competent peers. With time, they recognize the complexity of their work that they failed to appreciate initially, and their confidence drops.[11] This dip in personal accomplishment scores in SRNA2s and SRNA3s could be explained by this phenomenon.
The development and publication of a two-part podcast series demonstrates podcasts as convenient, engaging, and cost-effective when utilized to disseminate educational material and resources to anesthesia providers. Shifrin identified that with the rise of screen-based educational materials, podcasts can be an engaging alternative for adult learners to meet educational objectives.[12] This project implemented two virtual podcast sessions via Apple Podcasts and Spotify to report survey results and introduce mobile mindfulness as a feasible option to decrease stress and mitigate burnout. Podcasts were chosen to engage CRNAs and SRNAs in a modern, convenient way and to allow listeners to access the content on their own time. This project utilized results of the “Wellness Survey” to develop the topics of discussion for a two-part podcast series. These episodes revealed the results of the Maslach Burnout Inventory to listeners and delivered evidence-based resources to help mitigate burnout. The podcast achieved 112 total listens, 26 hours of total listening time, and an average of 22 minutes of play time per listen as provided by the analytic tool on Apple and Spotify Podcasts. A future project is in development to create further podcast episodes to address perception and management of burnout. Anecdotally, the podcasts did spur conversation and raise consciousness of the deleterious effects of burn out among nurse anesthesia providers.
Awareness of the CRNA and SRNA burnout experience at a large academic medical center underscores the importance of ongoing interventions to help mitigate instances of burnout within the profession and its training pipeline. Increasing knowledge of burnout implications on provider wellbeing, patient care, and healthcare delivery is the first step toward improvement.
Authors contributions
All authors were equally responsible for study design, data collection, manuscript creation and revising. All authors read and approved the final manuscript.
Funding
This work was supported by the University of Cincinnati College of Nursing Doctorate of Nursing Practice Project Fund. Funding was used to purchase the licensing agreement for use of the validated tool.
Conflicts of Interest Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Informed consent
Obtained.
Ethics approval
The Publication Ethics Committee of the Association for Health Sciences and Education. The journal’s policies adhere to the Core Practices established by the Committee on Publication Ethics (COPE).
Provenance and peer review
Not commissioned; externally double-blind peer reviewed.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Data sharing statement
No additional data are available.
Acknowledgements
Not applicable.
References
- Vells B, Midya V, Prasad A. Experiences of burnout among nurse anesthetists. OJIN. 2021;26(2). doi:10.3912/OJIN.Vol26No02PPT41
- Maslach C, Jackson S. The measurement of experienced burnout. J Organ Behav. 1981;2(2):99-113. doi:10.1002/job.4030020205
- Balayssac D, Pereira B, Virot J. Burnout, associated comorbidities and coping strategies in French community pharmacies—BOP study: A nationwide cross-sectional study. PLoS One. 2017;12(8):e0182956. PMID:28800612 doi:10.1371/journal.pone.0182956
- Mahoney C, Lea J, Schumann P. Turnover, burnout, and job satisfaction of Certified Registered Nurse Anesthetists in the United States: Role of job characteristics and personality. AANA J. 2020;88(1):39-48.
- de Oliveira G Jr, Chang R, Fitzgerald P. The prevalence of burnout and depression and their association with adherence to safety and practice standards: A survey of United States anesthesiology trainees. Anesth Analg. 2013;117(1):182-193. PMID:23687232 doi:10.1213/ANE.0b013e3182917da9
- Maslach C, Jackson S, Leiter M. Maslach Burnout Inventory. Scarecrow Education. 1997.
- Poghosyan L, Aiken L, Sloane D. Factor structure of the Maslach Burnout Inventory: An analysis of data from large scale cross-sectional surveys of nurses from eight countries. Int J Nurs Stud. 2009;46(7):894-902. PMID:19362309 doi:10.1016/j.ijnurstu.2009.03.004
- Maslach C, Jackson S. MBI - Human Services Survey for Medical Personnel - MBI-HSS (MP). Mind Garden. 2016.
- Maslach C, Leiter M. The problem with cut-offs for the Maslach Burnout Inventory. Mind Garden. 2018. https://www.mindgarden.com/documents/MBI-Cutoff-Caveat.pdf
- Kruger J, Dunning D. Unskilled and unaware of it: How difficulties in recognizing one’s own incompetence lead to inflated self-assessments. J Pers Soc Psychol. 1999;77(6):1121-1134. PMID:10626367 doi:10.1037/0022-3514.77.6.1121
- Rahmani M. Medical trainees and the Dunning-Kruger effect: When they don’t know what they don’t know. J Grad Med Educ. 2020;12(5):532-534. PMID:33149817 doi:10.4300/JGME-D-20-00134.1
- Shifrin M. Everyone is listening: Podcasts as an innovative educational approach in graduate level education. J. Nurs. Educ. 2024;63(10):1-3.
 This work is licensed under a
This work is licensed under a 