1.Introduction
Clinical placement has become increasingly complex due to the high demand for clinical spaces for students and the lack of available staff at facilities for student supervision or experiences.[1] The shortage of available clinical opportunities influences student progression, development, and learning. Upon graduation from nursing school, clinical facilities expect new graduates to enter nursing practice possessing the skills and knowledge to deliver safe, effective, high-quality care.[2] Numerous studies and reports have indicated that new graduates are not prepared to enter the nursing workforce at the novice level.[2—4] Although nurse residency programs are widely implemented to support the transition to practice following graduation, undergraduate clinical education remains the primary setting in which students develop foundational clinical skills, judgment, and professional identity. Strengthening clinical education at the undergraduate level is therefore essential to prepare graduates for both initial practice and subsequent transition-to-practice programs.[5] Schroers et al. report that only 9% of new graduates were prepared to enter clinical practice in 2020.[6] New graduate nurses make more errors as a direct result of poor decision-making and errors in clinical judgment.[3] This integrative review aimed to explore and critically analyze the clinical experiences of undergraduate nursing students in generalist nurse clinical placements in the United States.
1.1Background
Clinical education is a required component of undergraduate nursing education and a prerequisite for program completion and licensure.[1,6] Clinical education encompasses hands-on experiences with face-to-face patient contact in healthcare environments, such as hospitals, clinics, or community settings.[4,7,8] During clinical experiences, students complete a specified number of direct patient care hours, during which they are exposed to practical nursing skills and acquire the knowledge, professional behaviors, and attitudes necessary for success as practicing nurses.
There are several traditional clinical education models used by nursing programs.[1,4,9] In the faculty supervision model, clinical faculty accompany small groups of students to clinical units.[10] The assigned clinical faculty or clinical instructor is responsible for all learning activities and provides expert supervision and guidance of patient care activities.[6] Clinical faculty must balance the educational needs of students with the operational demands of the clinical unit, often while supervising up to ten students simultaneously.[10,11] A key strength of this model is the presence of an academic nurse educator who can intentionally link classroom content with clinical learning.[12] However, limited faculty availability may result in task-focused supervision rather than deeper integration of knowledge, skills, and professional judgment.[4]
Another model, the preceptorship model, assigns students to a nurse preceptor employed by the facility on the student’s assigned unit.[1,6,13] The preceptorship model provides one-on-one supervision, where the preceptor is responsible for all learning activities for the student. The preceptor provides oversight of patient care decisions and assessments, as well as expert supervision of patient care. A strength of this model is the student’s opportunity to practice and learn alongside an experienced nurse with one-on-one supervision.[12] A significant weakness of this model is that preceptors are often not trained as educators and may struggle to bridge the gap between classroom and clinical learning.[7,12] Additionally, preceptors may experience workload burden, limited time for teaching, and lack of compensation, all of which can reduce their availability to students and contribute to variability in clinical learning experiences.
Alternative clinical education models include Dedicated Education Units (DEUs) and hub-and-spoke models, both of which rely on structured academic–practice partnerships.[1,14] DEUs are intentionally designed clinical units in which staff nurses are prepared and supported to serve as clinical educators while academic faculty assume a coaching and oversight role. This model emphasizes consistency, shared educational responsibility, and intentional integration of learning objectives within the clinical environment. DEUs have been described as a strategy to enhance student engagement, increase instructor availability, and strengthen the integration of classroom learning with clinical practice.[1,12]
Hub-and-spoke models organize clinical education around a central “hub” facility, typically a large healthcare organization or academic medical center.[1,14] From the “hub” facility, there are affiliated “spoke” sites such as community hospitals, outpatient clinics, or specialty units. This model allows nursing programs to expand clinical placement capacity while maintaining curricular consistency and standardized learning outcomes across diverse settings. Both DEU and hub-and-spoke models require strong institutional collaboration, coordinated faculty involvement, and resource investment, which may limit feasibility for some nursing programs despite their potential to address clinical placement shortages and variability in student experiences.[1,8,12,14]
Simulation-based learning is also widely used in undergraduate nursing education as a component of clinical preparation.[4] Simulation supports the development of psychomotor skills, clinical judgment, and confidence by providing structured, low-risk opportunities for deliberate practice and feedback prior to and alongside in-person clinical experiences. When integrated intentionally, simulation can help students prepare for real-world clinical encounters. Although simulation plays an important adjunctive role in clinical education, it is designed to complement rather than fully replace direct patient care experiences required for licensure and professional practice.
Although clinical education is a long-standing requirement in nursing curricula, significant gaps remain in understanding its impact on student readiness and competence. Leighton et al. recently conducted a systematic review to examine traditional clinical outcomes.[4] The Leighton et al. review was empty, as the researchers found no current evidence to support conventional clinical education models. The primary purpose of clinical education is to prepare students for independent clinical practice by application of classroom knowledge to real-life patients.[15] The clinical experience fosters the advancement of student skills and confidence in the clinical setting.[2,16] Clinical education also promotes student socialization and integration into the nursing profession, influencing future career decisions.[1]
Understanding the current state of nursing clinical education is timely and relevant, given the persistent challenges facing the nursing workforce and the increasing demands for practice-ready graduates. The ongoing global nursing shortage, exacerbated by the COVID-19 pandemic and an aging population, has underscored the urgent need for effective clinical training models that can foster student competence, confidence, and professional identity.[5] Clinical education is a foundational rite of passage for nursing students.[16] There are several benefits to providing clinical education, including enhanced communication, increased student confidence, and improved student self-efficacy.[2,16] To address the current gap in clinical education in undergraduate nursing programs, the purpose of this study was to conduct a comprehensive review of the existing literature. This integrative review aimed to explore and critically review the experiences of undergraduate nursing students learning in generalist nurse clinical rotations in the United States.
1.2Design
This literature review followed the framework of Whittemore and Knafl for integrative reviews.[14] This method provided a detailed approach to conducting an integrated review, which included problem identification, a clearly defined literature search, critical evaluation of the literature, analysis and data extraction, and synthesis of the findings. The integrative review method allows for the review of both qualitative and quantitative research.[17]
2.Methods
Four electronic databases were searched for primary research articles. The following databases were searched: PubMed, CINAHL Complete, APA PsycINFO, and Web of Science. A search string was created for the research question using Medical Subject Headings (MeSH) terms. Search terms included nursing student and undergraduate or baccalaureate or bachelor and clinical rotation or clinical experience or nursing clinicals or clinical education and United States or America or North America. Additional search criteria for the review were studies written in English and limited to primary peer-reviewed research articles written between January 2019 and December 2024. The initial search did not yield sufficient results. The search was expanded to include research articles written between January 2014 and April 2024. Reference lists were reviewed for additional research not identified in the original search. The search was conducted from January to April in 2024.
2.1Inclusion criteria
Articles were included if they were primary peer-reviewed research studies, written in the English language, and peer reviewed. Additional inclusion criteria included studies that focused on generalist nurse clinical experiences in undergraduate nursing programs in the United States. Studies were included from traditional baccalaureate nursing programs, associate degree registered nursing programs, and accelerated registered nursing programs. The review included qualitative and quantitative research, mixed-methods, and retrospective research designs.
2.2Exclusion criteria
Articles were excluded if they included graduate programs, nursing programs, or clinical rotations outside of the United States, were written in languages other than English, or were articles older than ten years. Additionally, articles were excluded if they included virtual clinical experiences, didactic teaching, or simulation-based experiences, as these modalities cannot fully replace in-person clinical education required by state boards of nursing for licensure and to allow focused examination of traditional, in-person clinical experiences. Studies focused on gender-specific or patient-population–specific clinical experiences were excluded to maintain focus on generalist undergraduate clinical education, as specialized contexts involve distinct emotional, ethical, and instructional factors that limit comparability across studies. Literature reviews, opinion papers, and editorials were also excluded.
2.3Search analysis
The overall search yielded 257 published research studies. Figure 1 showed the PRISMA flow diagram for this study.[18] These were exported to EndNote,[19] where duplicates were excluded. A total of 79 published research studies remained. Examination of abstracts excluded 59 studies for failure to meet inclusion criteria, with 20 studies remaining for further review. Full texts of the remaining 20 studies were reviewed for inclusion. The author reviewed the reference lists of these studies, which yielded two additional research studies. Thirteen of the remaining studies were excluded following the in-depth review due to failure to meet the inclusion criteria.
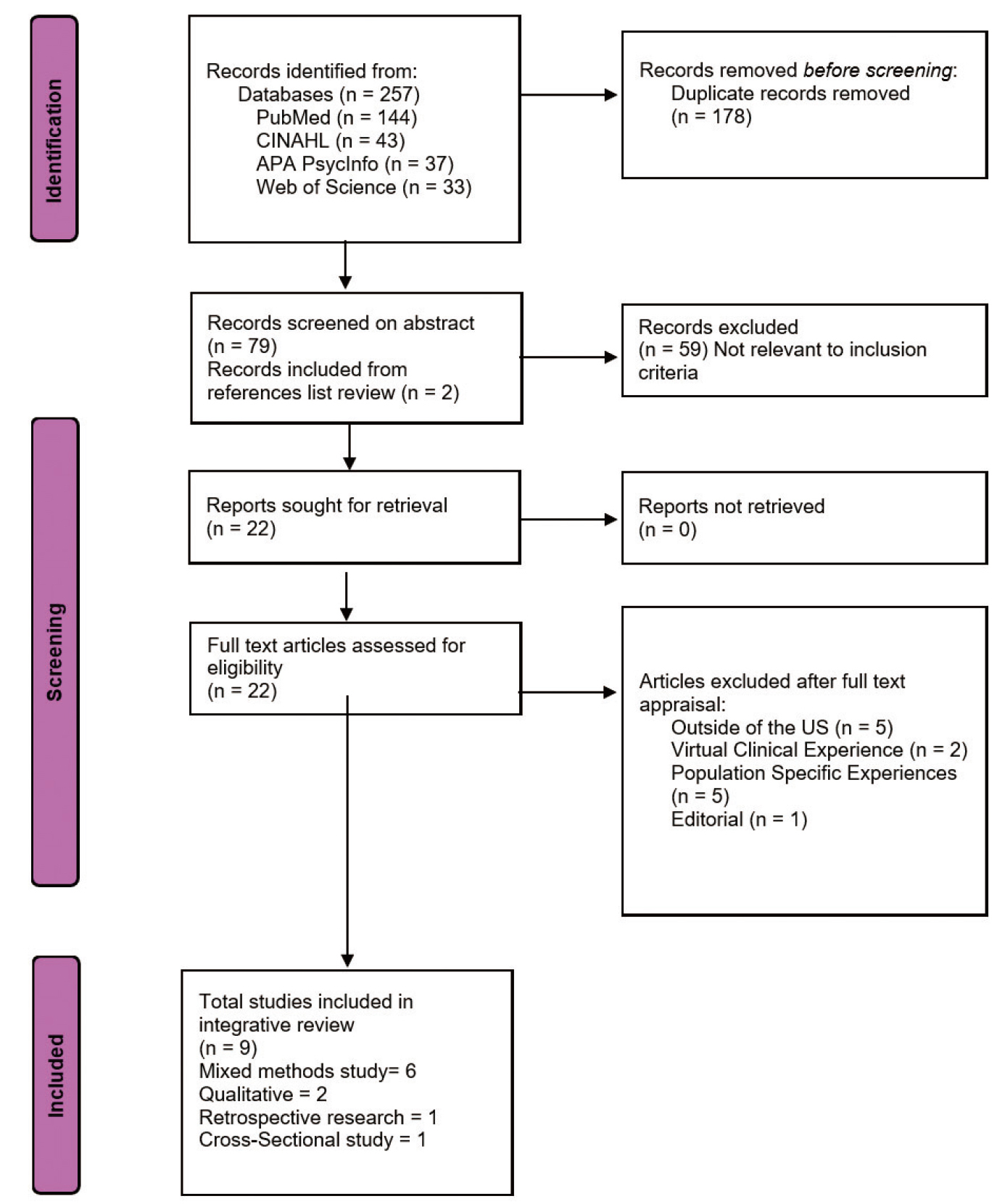
Figure 1.
PRISMA screening diagram
2.4Data extraction
A critical review of the remaining studies was completed using the Scoring System for Mixed Methods Research by Pluye et al.[20] This tool was used to screen studies for relevance, reliability, and applicability to the review. Following this final review, the definitive sample for this integrative review consisted of nine studies, which underwent critical appraisal: five mixed-method studies, two qualitative studies, one retrospective research study, and one cross-sectional study. Details of each included article were included in Table 1.
| Cowen, K.J., Hubbard, L.J., & Hancock, D.C. (2018). Expectations and experiences of nursing students in clinical courses: A descriptive study |
Examined nursing student feelings and expectations at beginning and end of clinical experiences, length of time to prep for clinical, and student learning styles | Southeastern US, Public University, junior level students n = 96 initial n = 72 follow up | Mixed methods Survey and follow up survey. 3 open- ended questions | Students were eager for hands-on experiences communication in both initial and follow up surveys. Students over estimated prep time. Learning became more refined. Learning styles were identified as primarily tactile and visual. |
Strengths: examined undergraduate baccalaureate clinical experiences. Limitations: limited to one university setting in southeastern US. Follow up survey had lower participation. |
| Cowen, K.J., Hubbard, L.J., & Hancock, D.C. (2016). Concerns of nursing students beginning clinical courses: A descriptive study. | Examined nursing student fears before and after their first clinical rotation and assessed confidence in physical assessment skills | Upper-level nursing students in a generic baccalaureate program n = 96 initial n = 72 follow up | Mixed methods Survey and follow up survey. 2 open-ended questions, ranking scale for confidence in physical assessment skill (0-100 mm) | Students have fears throughout nursing clinicals that impact performance in clinical settings. Confidence levels increased with clinical experience. | Strengths: examines undergraduate baccalaureate clinical experiences. Offers recommendations for faculty to mitigate and address fears of students. Limitations: Sample is not clearly defined. Students were in varied experiences. Survey questions not disclosed, rating scale for physical assessment unclear. Discussion does not operationalize “fears” of students. |
| Donovan, L.M., Strunk, J.A., Lam, C., Argenbright, C., Robinson, J., Leisen, M., & Puffenbarger, N. (2021). Enhancing the prelicensure clinical learning experience: A student-centered learning approach. | Examined the influence of clinical instructors on the clinical experiences of nursing students | Southeastern US BSN program Nursing students in final 2 years of program n = 194 | Mixed method cross-sectional survey design Qualitative and quantitative questions Modified CLEI tool |
Faculty approach of student-centeredness was highly valued by students. | Strengths: Explored student expectations of faculty in clinical environment which contributes to the student overall experience. Theoretical basis included (Student-centered learning theory). Study findings linked to theory. Weaknesses: Faulty experience and qualifications were not included or explored as a variable. No exclusion criteria listed. Study did not explore or define the concept of “student learning”. |
| George, T.P., DeCristofaro, C., & Murphy, P.F. (2020). Self-efficacy and concerns of nursing students regarding clinical experiences. |
Examined student perceptions of self-efficacy and student concerns in clinical rotations | Public, liberal arts university, southeastern US, Junior and senior level students, n = 112 initial n = 69 follow up | Mixed methods survey Qualitative and quantitative questions |
Data indicated an increase in student self-efficacy. Identified student preferences for learning. |
Strengths: examined experiences of BSN students in the US. Survey questions, themes, and student quotes included in tables. Weaknesses: Terminology for was not clearly defined. Low response rate in follow up survey. |
| Hood, T.L., & Copeland, D. (2021). Student nurses' experiences of critical events in the clinical setting: A grounded theory | Investigated nursing student experiences when critical events occur in the clinical setting | Midwestern US BSN and ADN students from 3 different 4-year universities n = 14 | Qualitative study | Ten concepts were identified in association with student experiences of critical events in the clinical setting. Offered recommendations for each theme for clinical faculty to better support students. | Strengths: explored nursing student experiences in the US. Theoretical model generated from this research. Participant safety provisions for critical events. Weaknesses: Small sample size. Multiple themes were identified by authors, discussion became confusing. |
| Payne, C. (2016). Transitions into practice: First patient care experiences of baccalaureate nursing students. | Explored initial clinical experiences of first semester baccalaureate nursing students | Southeastern US, 2 universities with 4-year baccalaureate programs (same state) n = 120 | Qualitative study Participants responded in writing to a single question |
Three themes were identified to describe student initial clinical experience. Each theme had identified sub-themes. Offered understanding of student clinical experience to improve future experiences. | Strengths: explored nursing student experiences in the US. Large sample size for qualitative study. Long study (3 years of data collection). Weaknesses: Clinical rotation varied in length, location, and setting. |
| Schroers, G., Shrikanth, S., & Pfiffer, J. (202). Undergraduate nursing student experiences in American clinical learning environment: A descriptive study. | Investigated undergraduate nursing student experiences in clinical settings, specifically focused on skills, supervision, and feedback | Midwestern US, private university ABSN students n = 496 | Descriptive retrospective research design | The number of clinical experiences and skills was limited. Supervision and feedback were not routinely provided. Recommended use of skills labs, simulation labs, and dedicated education units (DEUs) to increase student experiences. | Strength: explored nursing student experiences in the US Weaknesses: Sample was not defined by numbers of students, but rather in number of surveys completed. Some surveys were partially completed. Quality of clinical experiences was not explored. Clinical experiences were varied. |
| Singer, D.L., Zhang, Y., Baker, K.A., & Walker, D. (2024). Modifiable factors contributing to belongingness of undergraduate nursing students in the clinical learning environment: An exploratory study. | Assessed factors influencing a student's sense of belonging in the clinical environment | National Study through the NSNA database, nursing students who had completed at least one clinical course n = 759 | Cross-sectional study | Identified 11 factors for belongingness for nursing students in the clinical environment. Nursing students overall felt comfortable in clinical environments. The 11 factors were identified and recommended to clinical faculty to impact practice. | Strengths: explored nursing student experiences of belonging in the clinical environment in the US. Extensive study with large, diverse, national sample Weaknesses: Study was open only to NSNA members, excluding lower performing students or working students or those who may not participate in extracurricular activities. |
| Wallace, L., Bourke, M.P., Tormoehlen, L.J., & Poe-Greskamp, M.V. (2015). Perceptions of clinical stress in baccalaureate nursing students. |
Explored stress in nursing students in clinical experiences. | Single university in Midwest US, n = 65 | Mixed method Survey questions plus one qualitative question |
Students experienced stress in clinical environment related to new experiences, staff, or clinical instructor. Recommended for instructors to plan ahead and mitigate stressors when possible. |
Strengths: explored nursing student experiences in the US. Weaknesses: Small sample size. Focus is only on stress experiences, so questions may have only explored negative experiences. Survey questions not disclosed. |
3.Results
A data extraction was completed following the Whittemore and Knafl framework.[14] Similarities and differences were identified between the included studies (see Table 1). Four themes emerged from the critical analysis of the data: student emotional responses to clinical experiences, the influence of clinical instructors or nurse preceptors on student experiences, student confidence and sense of belonging in the clinical environment, and student clinical skill development. Additionally, it was noted that all studies included recommendations for nurse educators.
3.1Characteristics of studies
Themes and outcomes were depicted in Figure 2. A total of nine studies were used in this review. All studies were published between 2014 and 2024. All studies (n = 9) explored experiences of undergraduate nursing students in the clinical environment. Additionally, all studies involved nursing students pursuing a degree that would result in a career as a registered nurse. Nearly all studies (n = 8) specifically explored student clinical experiences in acute care settings. One study did not specify the location of the student’s clinical experiences. Seven studies included qualitative questions, with two being entirely qualitative studies. Only one study (n = 1) focused specifically on the influence of clinical instructors on the clinical experience of the student. All studies (n = 9) provided recommendations for nurse educators to enhance or improve students’ clinical experiences. Very few studies (n = 1) discussed student skill development in clinical experiences. Table 2 illustrates the thematic analysis of the studies in this review.
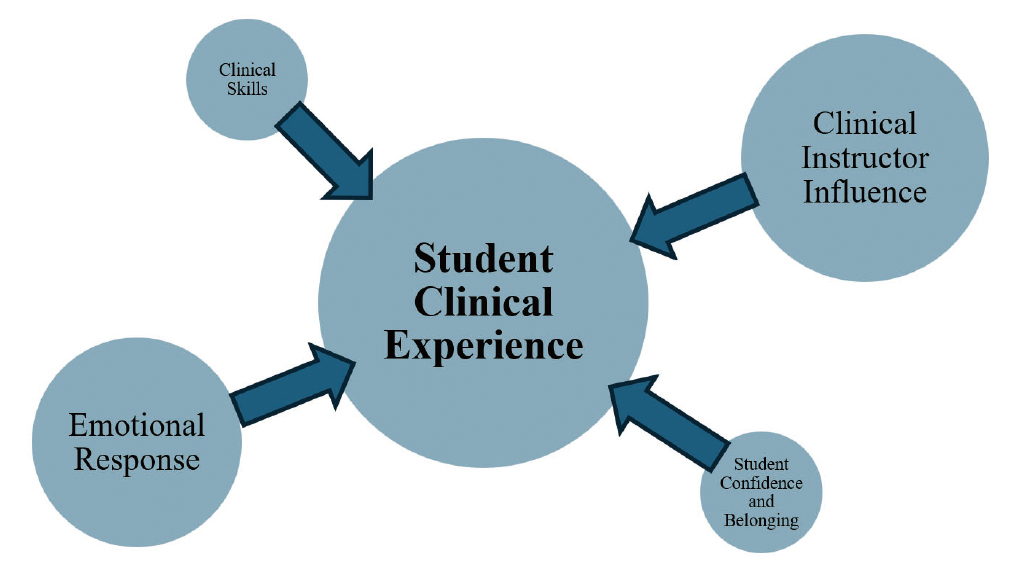
Figure 2.
Diagram of thematic analysis
| Cowen et al. (2018) | Yes | Yes | |||
| Cowen et al. (2016) | Yes | Yes | Yes | ||
| Donovan et al. (2022) | Yes | Yes | |||
| George et al. (2020) | Yes | Yes | Yes | Yes | |
| Hood & Copeland (2021) | Yes | Yes | Yes | ||
| Payne (2016) | Yes | Yes | Yes | ||
| Schroers et al. (2023) | Yes | Yes | Yes | ||
| Singer et al. (2024) | Yes | Yes | Yes | ||
| Wallace et al. (2015) | Yes | Yes | Yes |
3.2Student emotional response to clinical experiences
Six research studies explored the theme of students’ emotional responses to clinical experiences. The American Psychological Association (n.d.) defines emotional response as “an emotional reaction, such as happiness, fear, or sadness, to a given stimulus.” Studies that met this definition were included in this thematic analysis. The assessment of student emotional responses included excitement,[13,21] anxiety,[2,16] fear,[11,15,16] concern,[2,15] psychological distress or trauma,[14,21] stress,[11] nervousness,[16,21] and insecurities.[15,21] As clinical experiences increased, some students reported reduced fear,[16] and greater confidence.[8,15,16,22]
Most studies in the emotional response theme revealed adverse reactions such as stress, fear, anxiety, psychological distress, and nervousness associated with clinical experiences of undergraduate nursing students. These negative emotions may interfere with student development and learning.[15] Repeated negative feelings associated with the clinical learning environment were also reported to leave students questioning their decision to pursue a career in nursing.[21]
3.3Clinical instructor or nurse preceptor influence
Seventy-seven percent (n = 7) of the research studies included the theme of the influence of a clinical instructor or nurse preceptor on the clinical experience of the student. The research by Donovan et al. focused centrally on the impact of clinical faculty and nursing staff on the student experience in the clinical environment.[9] Researchers identified key behaviors that positively and negatively impacted student learning in the clinical environment. Key positive behaviors included communication, encouragement, and availability of clinical instructors. The key positive behaviors identified in this study align with findings in other studies reviewed, including George et al., Hood & Copeland, and Singer et al.[8,21,22]
In contrast, the study by Wallace et al. explored negative behaviors exhibited by clinical instructors and nurse preceptors.[11] These behaviors were more frequently reported as contributing to the student’s negative experiences. Nurse incivility, inconsistent instructor/preceptor expectations, and waiting for the clinical instructor/preceptor all created stress and anxiety in students. Payne reported similar findings regarding negative behaviors by clinical instructors and nurse preceptors, including a lack of interest in teaching, inadequate instructor organization, and bullying-type behaviors that impacted the students’ overall clinical learning experience.[16]
Both Payne and Singer et al. stressed the importance of a positive relationship between the clinical instructor and the clinical partner (hospital, clinic, or community health providers).[8,16] This relationship affected the learning environment and influenced the student experience.
3.4Student confidence and sense of belonging in clinical
Four studies contributed to the theme of student confidence and belonging in the clinical learning environment, each employing quantitative methods to assess variables such as confidence, self-efficacy, and sense of belonging. These traits are essential components of the overall student experience, influencing engagement and development in clinical settings.[8] Cowen et al. measured student confidence in physical assessment skills at two points during an academic semester, finding that initial confidence was low but improved with clinical exposure.[15] Similarly, George et al. examined self-efficacy, using a Likert scale to assess student confidence across 10 items at the beginning and end of a semester.[2] While students reported increased confidence in seven areas following the clinical experience, a significant decrease in response rate between data collection points raised concerns about the validity of the findings. Singer et al. explored students’ perceived sense of belonging in the clinical environment, reporting that a sense of belonging significantly influenced confidence and willingness to participate in learning activities.[8] This large-scale study (n = 759) highlighted that inclusion and belonging have a positive impact on students’ confidence and professional development. Finally, Leighton et al., in a literature review on student outcomes, noted that much of the existing research relies on student self-reports of clinical confidence and skill proficiency.[4] They cautioned that confidence and competence are not synonymous, as students often overestimate their abilities.
3.5Clinical skill development
This review included a single study that explored skill development. Quantitative data were collected on the number of psychomotor skills and physical assessments performed by students on each clinical day through self-report by students.[6] Data was also obtained about supervision and feedback. Researchers found that students had minimal experience in the clinical environment, particularly in psychomotor skills and physical assessment skills. Additionally, Schroers et al. indicated that the lack of hands-on opportunities contributes to the trend of graduates who are unprepared for clinical practice.[6] These findings were consistent with the results of the systematic review conducted by Leighton et al., which found no evidence to support our current clinical education model for teaching clinical skills.[4] Information regarding students’ prior laboratory or simulation-based learning experiences was inconsistently reported across included studies and therefore could not be systematically analyzed, though such experiences may influence students’ competence and confidence in clinical settings.[6]
4.Discussion
This integrative review examined recent literature on the clinical experiences of undergraduate nursing students in the United States. Four primary themes emerged: (1) student emotional responses to the clinical environment, (2) confidence and belonging, (3) the influence of the clinical instructor, and (4) gaps in clinical learning structure and content. Most studies focused on students’ perceptions and emotional experiences rather than the specific nature or quality of clinical learning activities. Despite the small sample, the focused scope allowed for in-depth synthesis of student experiences within comparable clinical contexts, strengthening interpretive coherence.
One notable finding was students’ enthusiasm for hands-on learning opportunities in clinical settings. Across several studies, students consistently reported excitement and eagerness to engage in real-world patient care.[6,13,15,16] While this aligns with the American Association of Colleges of Nursing (AACN) Essentials,[23] which identifies clinical learning as a core competency for entry-level practice, the literature provides little detail about how these experiences are structured or supervised. For example, Schroers et al. noted that it remains unclear whether qualified clinical educators effectively guide students’ hands-on experiences.[6] This lack of specificity is concerning, given that clinical education is central to the development of psychomotor skills, psychosocial competence, and clinical judgment. Faculty shortages and increasing reliance on adjunct or preceptor-based models may contribute to variability in supervision and student learning outcomes.
This review also highlighted a broader issue: the limited and inconsistent evidence base for best practices in clinical education. Despite expanding the search period to ten years, only nine relevant studies met the inclusion criteria. Leighton et al. highlighted this issue in their systematic review, concluding that the available evidence is insufficient to inform clinical education models or ensure consistency in clinical performance assessment.[4] Accrediting bodies provide few concrete guidelines on clinical content, the quantity and distribution of required clinical hours, or the appropriate balance between simulation-based and traditional placements, which further complicates the landscape for both educators and students.
Notably, all studies included in this review (n = 9) offered recommendations for enhancing clinical education. A substantial majority (n = 8) emphasized the importance of the student-instructor relationship as a critical factor in shaping positive learning experiences.[2,8,10,11,13,15,16,21] Additional recommendations focused on improving communication,[2,10,13,15] providing meaningful feedback to students,[8,21] and cultivating a supportive presence in clinical environments.[2,8,11,13,16] Only one study directly addressed the development of clinical skills, recommending the use of skills labs, simulation-based learning, and dedicated education units to strengthen practice readiness.[6] In undergraduate nursing education, psychomotor skill development is supported through a continuum of learning environments, including skills laboratories, simulation-based experiences, and structured clinical models such as Dedicated Education Units, which collectively provide opportunities for guided practice, consistent feedback, and progressive skill acquisition. These findings underscore the urgent need to invest in evidence-based clinical education models that promote both competence and confidence in nursing graduates.
Several limitations are worth noting in this study. A lack of available research in this area limits this integrative review. The inclusion and exclusion criteria for this integrative review were intentionally narrow to allow focused examination of undergraduate nursing students’ experiences in U.S.-based, in-person generalist clinical education. While this approach strengthened conceptual coherence across studies, it resulted in a limited sample size. Exclusion of international studies and simulation-based research further reduced the number of eligible articles, despite the existence of high-quality research in these areas. As a result, findings may not be generalizable to nursing education contexts outside the United States or to clinical education models that rely heavily on simulation.
Despite the limitations, the state of the science suggests critical areas for nursing research. Future research in clinical nursing education should move beyond students’ emotional and perceptual experiences to investigate the structural and pedagogical components that shape clinical learning. Specifically, studies are needed to examine how psychomotor skill development occurs within various clinical environments and under differing educational models. Research exploring the preparation and qualifications of clinical faculty, as well as the teaching methods they employ, could provide valuable insights into educator effectiveness and student outcomes. While the use of simulation as an adjunct to traditional clinical education is well established, continued inquiry into how simulation-based learning can best support student competency and readiness for practice is warranted.[24] Furthermore, future studies should investigate how students acquire and apply professional competencies during clinical placements, as well as how supervision models and learning environments impact these processes. A more comprehensive and evidence-informed understanding of clinical education is essential to guide curriculum development, inform policy, and ensure the adequate preparation of practice-ready nurses.
Implications for nursing education
Findings from this integrative review suggest that future clinical education in undergraduate nursing programs must move beyond traditional, loosely structured clinical placements toward more intentional and evidence-informed learning designs. Nursing educators and academic leaders should prioritize the development of clinical experiences that explicitly align learning objectives, supervision models, and expected student outcomes.
First, greater emphasis should be placed on preparation and support of clinical educators, including both academic faculty and nurse preceptors. Structured orientation, ongoing development in teaching strategies, and clear expectations for student supervision may enhance consistency in clinical instruction and improve student learning experiences. Investment in faculty development and academic–practice partnerships is particularly critical as programs increasingly rely on adjunct faculty and preceptor-based models.
Second, nursing programs should adopt a deliberate approach to clinical skill development by intentionally integrating skills laboratories, simulation-based learning, and in-person clinical experiences. Rather than viewing these components as separate or interchangeable, educators should design clinical curricula that support progressive skill acquisition, repeated practice, and timely feedback across learning environments. Structured clinical models, such as Dedicated Education Units, may offer opportunities to strengthen supervision, clarify expectations, and support hands-on skill development in authentic clinical settings.
Third, findings highlight the importance of relational and psychosocial aspects of the clinical learning environment, including student–instructor relationships, communication, feedback, and a sense of belonging. Clinical experiences should be designed to promote psychological safety and inclusion, as these factors influence student confidence, engagement, and willingness to participate in learning activities. Intentional strategies to foster supportive clinical environments may mitigate student anxiety and enhance professional identity formation.
Finally, nursing education leaders should critically examine clinical hour requirements and learning expectations, recognizing that the quantity of clinical hours alone does not ensure competence. Greater attention should be given to the quality, structure, and supervision of clinical experiences, as well as to how students demonstrate competence and readiness for practice. Collectively, these implications underscore the need for coordinated, evidence-based approaches to clinical education that better prepare undergraduate nursing students for professional practice.
5.Conclusion
Clinical nursing experiences are challenging to obtain, standardize, and study; however, their importance in preparing competent, practice-ready nurses is undeniable. These experiences provide critical opportunities for students to develop clinical judgment, reinforce theoretical knowledge, and build essential psychomotor skills.[6,12] This integrative review advances understanding of undergraduate nursing students’ internal responses to clinical learning and highlights the pivotal role of clinical instructors in shaping meaningful clinical experiences.
Findings from this review also reveal a persistent gap in the literature related to psychomotor skill development within clinical settings. Notably, only one included study directly examined clinical skill development, underscoring the need for further research in this area. Future investigations should focus on how undergraduate nursing students acquire and apply psychomotor skills across clinical learning environments, including examination of instructional strategies, supervision models, and learning contexts that support skill development. Strengthening this evidence base will require continued collaboration among nurse educators, clinical instructors, preceptors, and practice partners to inform evidence-based best practices in clinical education.
Authors contributions
Mrs. Orsburn led study design, data collection, and manuscript preparation. Dr. Lindley reviewed the manuscript and contributed critical revisions. All authors reviewed and approved the final version of the manuscript.
Funding
Funding for open access to this research was provided by University of Tennessee’s Open Publishing Support Fund.
Conflicts of Interest Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Informed consent
Obtained.
Ethics approval
The Publication Ethics Committee of the Association for Health Sciences and Education. The journal’s policies adhere to the Core Practices established by the Committee on Publication Ethics (COPE).
Provenance and peer review
Not commissioned; externally double-blind peer reviewed.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Data sharing statement
No additional data are available.
Acknowledgements
The authors would like to acknowledge Ms. Melanie Dixon and Ms. Niki Cobb, Health Sciences Librarians at the University of Tennessee, Knoxville, for their assistance.
References
- Forber J, DiGiacomo M, Carter B. In pursuit of an optimal model of undergraduate nurse clinical education: An integrative review. Nursing Education in Practice. 2016;21:83-92. doi:10.1016/j.nepr.2016.09.007
- George T, DeCristofaro C, Murphy P. Self-efficacy and concerns of nursing students regarding clinical experiences. Nurse Education Today. 2020;90:104401. doi:10.1016/j.nedt.2020.104401
- Jessee M. An update on clinical judgment in nursing and implications for education, practice, and regulation. Journal of Nursing Regulation. 2021;12(3):50-60. doi:10.1016/S2155-8256(21)00116-2
- Leighton K, Kardong-Edgren S, McNelis A. Traditional clinical outcomes in prelicensure nursing education: An empty systematic review. Journal of Nursing Education. 2021;60(3):136-142. doi:10.3928/01484834-20210222-03
- National Academies of Sciences, Engineering, and Medicine. The future of nursing 2020–2030: Charting a path to achieve health equity. Washington, DC; The National Academies Press. 2021. doi:10.17226/25982
- Schroers G, Shrikanth S, Pfieffer J. Undergraduate nursing student experiences in American clinical learning environment: A descriptive study. Nurse Education Today. 2023;129:105895. doi:10.1016/j.nedt.2023.105895
- Leighton K, McNelis A, Kardong-Edgren S. The competency of clinical nurse educators. Journal of Professional Nursing. 2022;43:1-4. doi:10.1016/j.profnurs.2022.08.004
- Singer D, Zhang Y, Baker K. Modifiable factors contributing to belongingness of undergraduate nursing students in the clinical learning environment: An exploratory study. Nurse Education Today. 2024;133:106065. doi:10.1016/j.nedt.2023.106065
- Clark J, Vander Riet P, Bowen L. Nurses and undergraudate student nurses’ experiences in collaborative clinical placement programs in acute hospitals: An integrative literature review. Nurse Education Today. 2020;95:104578. doi:10.1016/j.nedt.2020.104578
- Donovan L, Strunk J, Lam C. Enhancing the prelicensure clinical learning experience: A student-centered learning approach. Nurse Educator. 2022;47(2):108-113. doi:10.1097/NNE.0000000000001085
- Wallace L, Bourke M, Tormoehlen L. Perceptions of clinical stress in baccalaureate nursing students. International Journal of Nursing Education and Scholarship. 2015;12(1):91-98. doi:10.1515.ijnes-2014-0056
- Flood L, Robinia K. Bridging the gap: Strategies to integrate classroom and clinical learning. Nursing Education in Practice. 2014;14(4):329-332. doi:10.1016/j.nepr.2014.02.002
- Cowen K, Hubbard L, Hancock D. Expectations and experiences of nursing students in clinical courses: A descriptive study. Nurse Education Today. 2018;67:15-20. doi:10.1016/j.nedt.2018.04.024
- Whittemore R, Knafl K. The integrative review: Updated methodology. Journal of Advanced Nursing. 2005;52(5):546-553. doi:10.1111/j.1365-2648.2005.03621.x
- Cowen K, Hubbard L, Hancock D. Concerns of nursing students beginning clinical courses: A descriptive study. Nurse Education Today. 2016;43:64-68. doi:10.1016/j.nedt.2016.05.001
- Payne C. Transitions into practice: First patient care experiences of baccalaureate nursing students. Nurse Education in Practice. 2016;16(1):251-257. doi:10.1016/j.nepr.2015.09.011
- Dhollande S, Taylor A, Meyer S. Conducting integrative reviews: a guide for novice nursing researchers. Journal of Research in Nursing. ;26(5):427-438. doi:10.1177/1744987121997907
- Page M, McKenzie J, Bossuyt P. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. British Medical Journal. 2021;372:71. doi:10.1136/bmj.n71
- EndNote. EndNote 21 [Computer software]. Clarivate. 2025.
- Pluye P, Gagnon M, Griffiths F. A scoring system for appraising mixed methods research and concomitantly appraising qualitative, quantitative, and mixed methods primary studies in mixed studies reviews. International Journal of Nursing Studies. 2009;46(4):529-546. doi:10.1016/j.ijnurstu.2009.01.009
- Hood T, Copeland D. Student nurses’ experiences of critical events in the clinical setting: A grounded theory. Journal of Professional Nursing. 2021;37(5):885-893. doi:10.1016/j.profnurs.2021.07.007
- American Psychological Association (n.d.). Emotional response. In APA Dictonary of Psychology. 2024. https://dictionary.apa.org/emotional-response
- American Association of Colleges of Nursing. The Essentials: Core competencies for professional nursing education. 2021. https://www.aacnnursing.org/Portals/42/AcademicNursing/pdf/Essentials-2021.pdf
- Jeffries P. Simulation in nursing education: From conceptualization to evaluation. Lippincott, Williams, & Wilkins. 2020.
 This work is licensed under a
This work is licensed under a 